| Citation: |
MA Xiangmin, ZHANG Xiangmei, ZHOU Xinping, REN Xiaofei, ZHANG Weifang, LIU Yunjiang. Real-world Research of Trastuzumab and Pertuzumab Combined with Chemotherapy in Neoadjuvant Treatment of HER2-positive Breast Cancer[J]. Cancer Research on Prevention and Treatment, 2022, 49(1): 46-52. DOI: 10.3971/j.issn.1000-8578.2022.21.0802

|
To analyze the efficacy and safety of trastuzumab (H) and pertuzumab (P) combined with different chemotherapy regiments in neoadjuvant therapy for HER2-positive breast cancer.
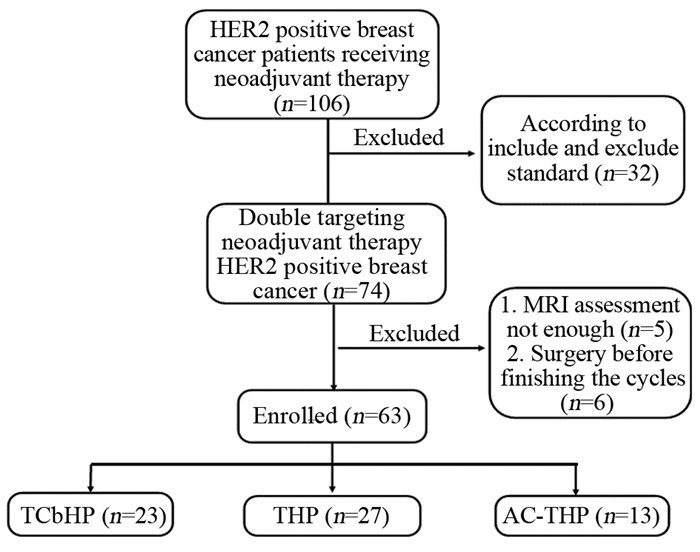
We retrospectively analyzed the clinical data of the patients with HER2-positive breast cancer who received HP combined with chemotherapy as neoadjuvant therapy and completed surgery. The primary endpoint was total pathologic complete response (tpCR) (ypT0/isypN0), the secondary endpoints were breast pathologic complete response(bpCR) (ypT0/is) and axillary pathologic complete response (apCR) (ypN0), and the factors influencing pCR were analyzed.
A total of 63 patients were included, of whom 23 were treated with TCbHP, 27 were treated with THP regimen, and 13 were treated with AC-THP. The overall tpCR rate was 65.1%, of which TCbHP was 73.9%, THP was 55.6%, and AC-THP was 69.2%. The tpCR rate of HR-negative patients was 79.2%, higher than that of HR-positive 56.4%. The overall bpCR rate was 69.8%, and apCR rate was 81.0%. Univariate analysis showed that HER2 status was a related factor affecting tpCR (P=0.023). The total effective rate by MRI was 87.3%. The level 3 and 4 toxicity of the TCbHP regimen was slightly higher than those of the THP and the AC-THP regimens.
HP combined with chemotherapy have achieved relatively high pCR. HER2 status is a related factor that affects tpCR. The adverse reactions are controllable.
Competing interests: The authors declare that they have no competing interests.
| [1] |
Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries[J]. CA Cancer J Clin, 2021, 71(3): 209-249. doi: 10.3322/caac.21660
|
| [2] |
Owens MA, Horten BC, Da Silva MM. HER2 amplification ratios by fluorescence in situ hybridization and correlation with immunohistochemistry in a cohort of 6556 breast cancer tissues[J]. Clin Breast Cancer, 2004, 5(1): 63-69. doi: 10.3816/CBC.2004.n.011
|
| [3] |
Ross JS, Slodkowska EA, Symmans WF, et al. The HER-2 receptor and breast cancer: ten years of targeted anti-HER-2 therapy and personalized medicine[J]. Oncologist, 2009, 14(4): 320-368. https://pubmed.ncbi.nlm.nih.gov/19346299/
|
| [4] |
Slamon DJ, Clark GM, Wong SG, et al. Human breast cancer: correlation of relapse and survival with amplifi-cation of the HER-2/neu oncogene[J]. Science, 1987, 235(4785): 177-182. doi: 10.1126/science.3798106
|
| [5] |
Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis[J]. Lancet, 2014, 384(9938): 164-172. doi: 10.1016/S0140-6736(13)62422-8
|
| [6] |
Hammond ME, Hayes DF, Dowsett M, et al. American Society of Clinical OncologyCollege Of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer[J]. J Clin Oncol, 2010, 28(16): 2784-2795. doi: 10.1200/JCO.2009.25.6529
|
| [7] |
Wolff AC, Hammond M, Allison KH, et al. HER2 Testing in Breast Cancer: American Society of Clinical OncologyCollege of American Pathologists Clinical Practice Guideline Focused Update Summary[J]. J Oncol Pract, 2018, 14(7): 437-441. doi: 10.1200/JOP.18.00206
|
| [8] |
Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RE-CIST guideline (version 11)[J]. Eur J Cancer, 2009, 45(2): 228-247. doi: 10.1016/j.ejca.2008.10.026
|
| [9] |
《乳腺癌新辅助治疗的病理诊断专家共识(2020版)》编写组. 乳腺癌新辅助治疗的病理诊断专家共识(2020版)[J]. 中华病理学杂志, 2020, 49(4): 296-304. doi: 10.3760/cma.j.cn112151-20200102-00007
Expert Consensus on pathologic Diagnosis of neoadjuvant therapy for Breast Cancer (2020 edition). Expert panel consensus on pathological diagnosis of breast cancer with neoadjuvant therapy, the 2020 version[J]. Zhonghua Bing Li Xue Za Zhi, 2020, 49(4): 296-304. doi: 10.3760/cma.j.cn112151-20200102-00007
|
| [10] |
Gianni L, Pienkowski T, Im YH, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial[J]. Lancet Oncol, 2012, 13(1): 25-32. doi: 10.1016/S1470-2045(11)70336-9
|
| [11] |
Schneeweiss A, Chia S, Hickish T, et al. Pertuzumab plus trastuzumab in combination with standard neoad-juvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: a randomized phase Ⅱ cardiac safety study (TRYPHAENA)[J]. Ann Oncol, 2013, 24(9): 2278-2284. doi: 10.1093/annonc/mdt182
|
| [12] |
Swain SM, Ewer MS, Viale G, et al. BERENICE Study Group. Pertuzumab, trastuzumab, and standard an-thracycline- and taxane-based chemotherapy for the neoadjuvant treatment of patients with HER2-positive local-ized breast cancer (BERENICE): a phase Ⅱ, open-label, multicenter, multinational cardiac safety study[J]. Ann Ocol, 2018, 29(3): 646-653.
|
| [13] |
Shao Z, Pang D, Yang H, et al. Efficacy, Safety, and Tolerability of Pertuzumab, Trastuzumab, and Docet-axel for Patients With Early or Locally Advanced ERBB2-Positive Breast Cancer in Asia: The PEONY Phase 3 Randomized Clinical Trial[J]. JAMA Oncol, 2020, 6(3): e193692. doi: 10.1001/jamaoncol.2019.3692
|
| [14] |
Gianni L, Pienkowski T, Im YH, et al. 5-year analysis of neoadjuvant pertuzumab and trastuzumab in patients with locally advanced, inflammatory, or early-stage HER2-positive breast cancer (NeoSphere): a multicentre, open-label, phase 2 randomised trial[J]. Lancet Oncol, 2016, 17(6): 791-800. doi: 10.1016/S1470-2045(16)00163-7
|
| [15] |
Nitz UA, Gluz O, Christgen M, et al. De-escalation strategies in HER2-positive early breast cancer (EBC): final analysis of the WSG-ADAPT HER2+/HR- phase Ⅱ trial: efficacy, safety, and predictive markers for 12 weeks of neoadjuvant dual blockade with trastuzumab and pertuzumab±weekly paclitaxel[J]. Ann Oncol, 2017, 28(11): 2768-2772. doi: 10.1093/annonc/mdx494
|
| [16] |
Hurvitz SA, Martin M, Symmans WF, et al. Neoadjuvant trastuzumab, pertuzumab, and chemotherapy versus trastuzumab emtansine plus pertuzumab in patients with HER2-positive breast cancer (KRISTINE): a random-ised, open-label, multicentre, phase 3 trial[J]. Lancet Oncol, 2018, 19(1): 115-126. doi: 10.1016/S1470-2045(17)30716-7
|
| [17] |
Hurvitz SA, Martin M, Jung KH, et al. Neoadjuvant Trastuzumab Emtansine and Pertuzumab in Human Ep-idermal Growth Factor Receptor 2-Positive Breast Cancer: Three-Year Outcomes From the Phase Ⅲ KRISTINE Study[J]. J Clin Oncol, 2019, 37(25): 2206-2216. doi: 10.1200/JCO.19.00882
|
| [18] |
González-Santiago S, Saura C, Ciruelos E, et al. Real-world effectiveness of dual HER2 blockade with per-tuzumab and trastuzumab f or neoadjuvant treatment of HER2-positive early breast cancer (The NEOPETRA Study)[J]. Breast Cancer Res Treat, 2020, 184(2): 469-479. doi: 10.1007/s10549-020-05866-1
|
| [19] |
Singh JC, Mamtani A, Barrio A, et al. Pathologic Complete Response with Neoadjuvant Doxorubicin and Cyclophosphamide Followed by Paclitaxel with Trastuzumab and Pertuzumab in Patients with HER2-Positive Early Stage Breast Cancer: A Single Center Experience[J]. Oncologist, 2017, 22(2): 139-143. doi: 10.1634/theoncologist.2016-0268
|
| [20] |
程元甲, 徐玲, 叶京明, 等. 帕妥珠单抗与曲妥珠单抗联合化疗在早期乳腺癌新辅助治疗中的疗效评价[J]. 中华临床医师杂志(电子版), 2020, 14(5): 344-348. doi: 10.3877/cma.j.issn.1674-0785.2020.05.005
Cheng YJ, Xu L, Ye JM, et al. Therapeutic effects of chemotherapy combined with pertuzumab and trastuzumab in neoadjuvant treatment of early breast cancer[J]. Zhonghua Lin Chuang Yi Shi Za Zhi(Dian Zi Ban), 2020, 14(5): 344-348. doi: 10.3877/cma.j.issn.1674-0785.2020.05.005
|
| [21] |
Spring L, Niemierko A, Haddad S, et al. Effectiveness and tolerability of neoadjuvant pertuzumab-containing regimens for HER2-positive localized breast cancer[J]. Breast Cancer Res Treat, 2018, 172(3): 733-740. doi: 10.1007/s10549-018-4959-8
|
Figures(1) / Tables(5)

This work is licensed under a Creative Commons Attribution 3.0 License.
Copyright © Editorial Department of Cancer Prevention Research 鄂公网安备 42011102005013号 鄂ICP备2022015867号
Supported by: Beijing Renhe Information Technology Co., Ltd. 
 DownLoad:
DownLoad: