
Comparison of Diagnostic Performance Between PI-RADS v2.1 and PI-RADS v2 for Prostate Cancer: A Meta-analysis
-
摘要:目的
对PI-RADS v2.1与PI-RADS v2在检测有临床意义的前列腺癌(csPCa)中的诊断性能进行Meta分析。
方法以“PIRADS v2.1”或“PI-RADS v2.1”为关键词检索CNKI、CBM、Medline、Embase等数据库所有文献。使用诊断准确性研究质量评估工具(QUADAS-2)进行文献质量评价,使用STATA17.0和ReMan5.4软件进行Meta分析。使用森林图表示每项研究的PI-RADS v2.1与PI-RADS v2的敏感度、特异性,并对敏感度、特异性、阳性似然比、阴性似然比、诊断比值比进行合并,以综合受试者工作特征曲线(SROC)对诊断性能进行评估。对肿瘤位置、不同阈值、作者国籍进行亚组分析。
结果共纳入12项研究,3158例患者,3243个病灶。PI-RADS v2.1在检测所有分区及整个腺体csPCa性能的SROC曲线下面积(AUC)较大。亚组分析显示:PI-RADS v2.1在检测移形带csPCa性能的SROC曲线下面积(AUC)较大;阈值为4时和中国的研究中PI-RADS v2.1在检测csPCa性能的SROC曲线下面积(AUC)最大。
结论与PI-RADS v2相比,PI-RADS v2.1在检测有临床意义的csPCa中,诊断性能并没有显著提高,总体特异性仍较低。
-
关键词:
- PI-RADS v2.1 /
- Meta分析 /
- 前列腺癌
Abstract:ObjectiveTo compare the diagnostic performance of PI-RADS v2.1 and PI-RADS v2 in the detection of clinically significant prostate cancer(csPCa) by Meta-analysis.
MethodsThe major biomedical databases were searched (CNKI, CBM, Medline, and Embase) with the keywords "PIRADS v2.1" or "PI-RADS v2.1". The Quality Assessment of Diagnostic Accuracy Studies Tool v2 (QUADAS-2) was used to evaluate literature quality. Meta-analysis was performed using STATA17.0 and ReMan5.4 software. Forest plots were used to represent the sensitivity and specificity of PI-RADS v2.1 and PI-RADS v2 for each study. Sensitivity, specificity, positive likelihood ratio, negative likelihood ratio, and diagnostic odds ratio were combined, and diagnostic performance was evaluated using asummary receiver operating characteristic curve (SROC). Subgroup analysis was performed on three covariables: tumor location, threshold, and the nationality of authors.
ResultsA total of 12 studies were included, involving 3 158 patients and 3 243 lesions. Forall zones and the whole gland, PI-RADS v2.1 had a larger area under the SROC curve (AUC) for csPCa performance, compared with PI-RADS v2. Subgroup analysis: PI-RADS v2.1 also had a larger area under the SROC (AUC) to detect transitional zone csPCa. Different diagnostic thresholds: when a score of 4 was used for the threshold, PI-RADS v2.1 had the maximum area under SROC (AUC) for csPCa performance detection. Author nationality: Researches of PI-RADS v2.1 in Chinese authors had the largest area under the SROC (AUC) in detecting csPCa performance.
ConclusionCompared with PI-RADS v2, the diagnostic performance of PI-RADS v2.1 in detecting csPCa is not obviously improved and overall specificity is still low.
-
Key words:
- PI-RADS v2.1 /
- Meta-analysis /
- Prostate cancer
-
0 引言
MRI已成为临床可疑前列腺癌(prostate cancer, PCa)患者的重要检测工具。MRI引导前列腺穿刺活检可以提高有临床意义的前列腺癌(clinically significant prostate cancer, csPCa)的检测准确性[1]。目前,前列腺影像报告和数据系统(prostate imaging-reporting and data system, PI-RADS)是解释前列腺MRI不可或缺的一部分,其目的是对前列腺癌进行风险分层,以指导组织学检查以及临床治疗方法的选择。自从2012年PI-RADS v1发表以来,2015年对其进行了重大修订(PI-RADS v2),但PI-RADS v2仍表现出一些局限性,比如观察者间的一致性只有良好到中等,对移行带(transition zone, TZ)前列腺癌的诊断准确性不高。因此2019年对PI-RADS v2再次进行了修订(PI-RADS v2.1),旨在为MRI解释提供更精确的定义,以减少观察者之间的差异,提高诊断准确性,特别是对于TZ病变[2]。Linhares Moreira[3]等学者研究显示PI-RADS v2.1诊断性能没有显著提高,然而Wang等[4]学者的研究显示PI-RADS v2.1在诊断csPCa的特异性显著降低,Oerther等[5]学者研究则表明,PI-RADS v2.1在评估TZ病变方面特异性和准确性明显高于PI-RADS v2。因此,PI-RADS v2.1的诊断性能仍然存在不确定性。因此,本研究拟对文献进行Meta分析,评价PI-RADS v2.1和PI-RADS v2在检测csPCa方面的诊断性能。
1 资料与方法
1.1 文献检索与筛选
检索中国知网(CNKI)、万方数据库、中国生物医学文献数据库(CBM)、Medline、Embase、Web of Science、Cochrane Library数据库,检索时间从建库至2022年4月16日。检索词为“PIRADS 2.1”或“PIRADSv 2.1”或“PI-RADS 2.1”或“PI-RADS v2.1”等,采用主题词加自由词对数据库进行文献检索,结合人工检索,并对纳入文献的参考文献进行二次检索。
由三位医师进行文献检索和初始标题/摘要审查,然后由两位医师阅读全文后以协商一致方式进行文献筛选,如仍不能达成一致,由经验更丰富的两位医师共同加入,共四位医师协商一致。不符合纳入标准的研究,如与研究目标相关,仍保留供一般审查和参考。
纳入标准分为主要标准和次要标准。主要标准:(1)PI-RADS v2.1与PI-RADS v2诊断性能比较的相关研究;(2)PI-RADS v2.1与PI-RADS v2在前列腺癌诊断方面的敏感度(sensitivity, SEN)、特异性(specificity, SPE)、阳性预测值(positive predictive value, PPV)和阴性预测值(negative predictive value, NPV)的研究;(3)文献构建2×2列联表,提供真阳性(true positive, TP)、假阳性(false positive, FP)、假阴性(false negative, FN)、真阴性(true negative, TN)数据,或提供足够的数据可以计算以上数据。次要标准:(4)关于PI-RADS v2.1和PI-RADS v2的观察者间一致性的研究;(5)提供PI-RADS v2.1和PI-RADS v2的PI-RADS有关类别csPCa比率。满足主要纳入标准(1)(2)(3),但不符合次要纳入标准(4)和(5)的研究也被纳入本研究。
排除标准:(1)会议论文、病例报道、评论、综述以及Meta分析;(2)不符合主要纳入标准的研究;(3)样本量小于30的研究。
1.2 数据提取
数据提取与合成由四名医师根据《Cochrane干预措施系统性评审手册》和《系统评价与荟萃分析首选报告项目》(PRISMA)检查表中的指南进行。
数据提取根据预先设计的表格进行数据提取,数据包括患者人口统计学、血清PSA、样本量、MRI扫描仪强度、DWI最高b值、观察者人数、前列腺分区和参考标准。PI-RADS v2.1和PI-RADS v2的TP、FP、FN和TN计数直接或通过重新计算从每项研究中得出,构建2×2列联表。
1.3 文献质量评价
由研究员根据QUADAS-2对纳入的研究进行质量评价,如仍不能达成一致,由经验更丰富的医师加入,协商一致。
1.4 统计学方法
使用STATA软件(Stata/MP 17.0)和ReMan(Review Manager 5.4.1)进行Meta分析。使用森林图表示每项研究的PI-RADS v2.1与PI-RADS v2的敏感度、特异性,并对SEN、SPE、阳性似然比(positive likelihood ratio, PLR)、阴性似然比(negative likelihood ratio, NLR)、诊断比值比(diagnostic odds ratio, DOR)进行合并,以综合受试者工作特征曲线(summary receiver operator characteristic curve, SROC)表示。对三个协变量:肿瘤位置(移行带)、阈值(阈值3与阈值4)、作者国籍(中国与外国)进行亚组分析。
2 结果
2.1 数据库检索结果
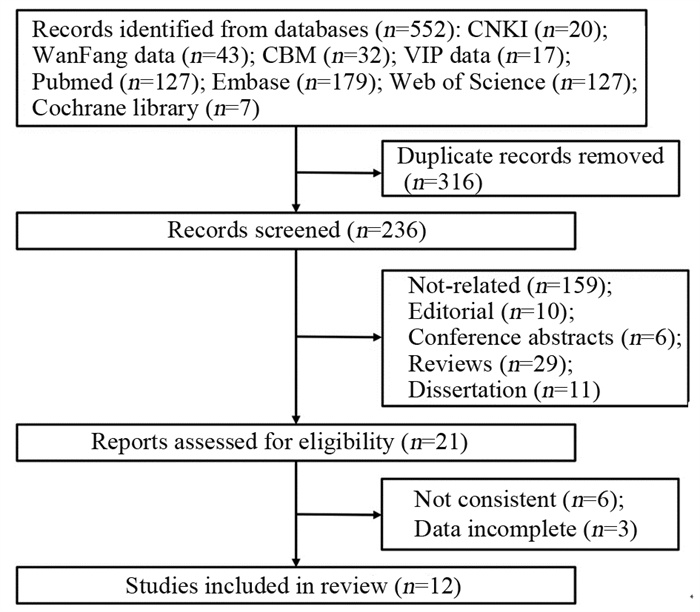
共检索到文献552篇,中文112篇、英语440篇,去除重复文献后共236篇,通过阅读标题与摘要排除215篇(不相关文献159篇,综述29篇,评论10篇、会议论文6篇、学位论文11篇)。选择21项研究进行全文阅读,其中6篇与研究内容不相符被排除,3篇数据不完整被排除,最终共12项研究被纳入Meta分析,文献筛选流程见图 1。
2.2 纳入文献的基本特征
12项研究共纳入3 158例患者,3 243个病灶。患者年龄41~86岁,血清PSA 0.5~129.3 ng/ml。
纳入的12项研究,对PI-RADS v2.1与PI-RADS v2在csPCa诊断性能方面进行了研究,其中6项关于TZ研究,1项研究外周带(peripheral zone, PZ),2项研究PZ、TZ及总病变,3项研究没有进行分区。
所有研究均为回顾性研究,7项研究以PI-RADS评分3~5分为阳性,1~2分为阴性;5项研究以PI-RADS评分4~5分为阳性,1~3分为阴性。所有研究都通过穿刺活检或前列腺切除术组织学诊断,以病理结果作为诊断标准,Gleason(GS)评分≥7和(或)体积≥0.5 cm3和(或)包膜外侵犯的病灶定义为csPCa。文献特征见表 1。
表 1 纳入Meta分析的12项研究的基本特征Table 1 Basic characteristics of 12 studies in the Meta-analysis
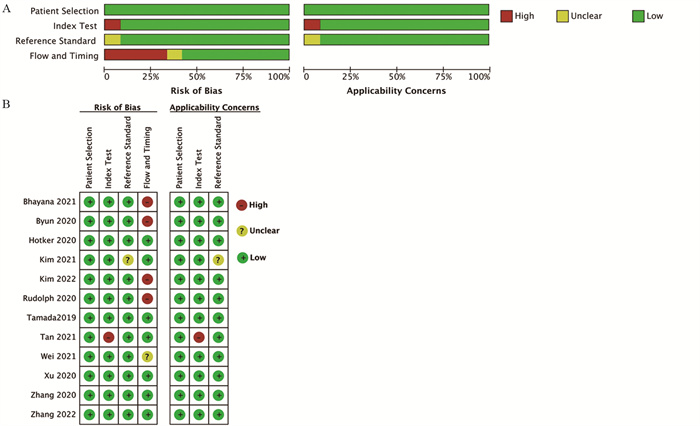
使用诊断准确性研究质量评估工具(QUADAS-2)对文献进行质量评价,见图 2。
![]() 图 2 QUADAS-2质量评价Figure 2 QUADAS-2 assessmentA: QUADAS-2 overall assessment included studies; B: QUADAS-2 assessment of all individuals included studies.
图 2 QUADAS-2质量评价Figure 2 QUADAS-2 assessmentA: QUADAS-2 overall assessment included studies; B: QUADAS-2 assessment of all individuals included studies.2.3 PI-RADS v2与PI-RADS v2.1对前列腺癌的诊断性能分析
2.3.1 整个腺体(包括PZ、TZ、ALL)诊断性能
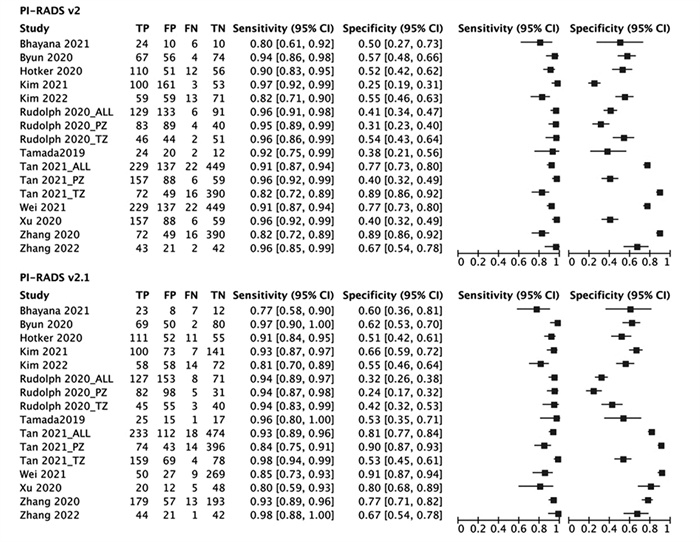
对所有分区及整个腺体(包括PZ、TZ、ALL)共12项研究3 243处病变,所有纳入单个研究PI-RADS v2与PI-RADS v2.1诊断准确性的敏感度均较高,总体敏感度分别为0.93(0.80~0.96)和0.93(0.77~0.98);特异性均稍低,总体特异性分别为0.53(0.25~0.89)和0.61(0.24~0.91),纳入的每个研究详细敏感度、特异性,见图 3。PI-RADS v2的总体敏感度、总体阴性似然比与PI-RADS v2.1比较差异较小,PI-RADS v2的总体特异性、总体阳性似然比、总体诊断比值比比PI-RADS v2.1略低,见表 2。与PI-RADS v2相比,PI-RADS v2.1在所有分区及整个腺体检测csPCa性能的SROC曲线下面积(area under curve, AUC)较大,见图 4A。
![]() 图 3 所有分区PI-RADS v2.1与PI-RADS v2诊断性能森林图Figure 3 Forest maps of diagnostic performance of PI-RADS v2.1 and PI-RADS v2 for all zones表 2 PI-RADS v2.1 vs. PI-RADS v2对整个腺体及移形带csPCa的诊断性能(95%CI)Table 2 Diagnostic performance of PI-RADS v2.1 vs. PI-RADS v2 for the whole gland and transition zone csPCa (95%CI)
图 3 所有分区PI-RADS v2.1与PI-RADS v2诊断性能森林图Figure 3 Forest maps of diagnostic performance of PI-RADS v2.1 and PI-RADS v2 for all zones表 2 PI-RADS v2.1 vs. PI-RADS v2对整个腺体及移形带csPCa的诊断性能(95%CI)Table 2 Diagnostic performance of PI-RADS v2.1 vs. PI-RADS v2 for the whole gland and transition zone csPCa (95%CI)
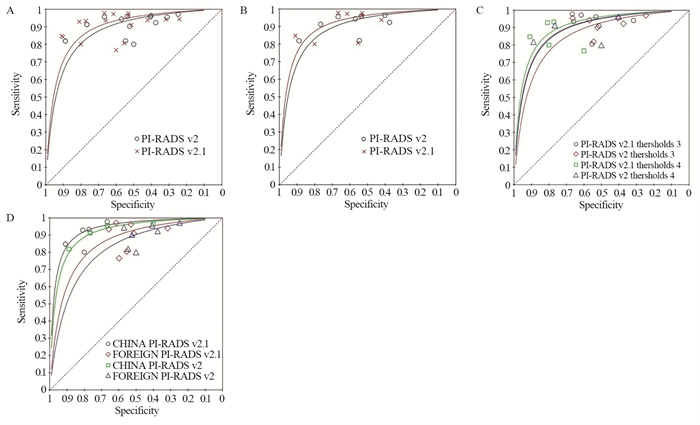
![]() 图 4 PI-RADS v2.1 vs. PI-RADS v2诊断性能SROC曲线Figure 4 SROC curves of diagnostic performance ofPI-RADSv2.1 vs. PI-RADSv2A: SROC curves of all zones and whole gland; B: SROC curves of transition zone; C: SROC curves of different threshold; D: SROC curves of different nationalities.
图 4 PI-RADS v2.1 vs. PI-RADS v2诊断性能SROC曲线Figure 4 SROC curves of diagnostic performance ofPI-RADSv2.1 vs. PI-RADSv2A: SROC curves of all zones and whole gland; B: SROC curves of transition zone; C: SROC curves of different threshold; D: SROC curves of different nationalities.2.3.2 肿瘤部位(分区)诊断性能亚组分析
(1)TZ区诊断性能:纳入TZ研究共8项2 205处病变。PI-RADS检测移形带前列腺癌与整个腺体诊断性能基本相同,PI-RADS v2的总体敏感度、总体阴性似然比与PI-RADS v2.1差异较小,PI-RADS v2的总体特异性、总体阳性似然比、总体诊断比值比比PI-RADS v2.1略低,见表 2。与PI-RADS v2相比,PI-RADS v2.1在检测TZ区csPCa性能的SROC曲线下面积(AUC)较大,见图 4B。(2)PZ区诊断性能:纳入PZ研究共3项1 513处病变,由于STATA软件metandi命令要求至少4项研究才能合并分析,因此未能合并诊断性能指标和也未绘制SROC曲线。
2.3.3 不同阈值(阈值为3 vs. 阈值为4)诊断性能亚组分析
共7项研究采用阈值3,采用阈值3时,PI-RADS v2.1总体敏感度较PI-RADS v2没有明显提高;PI-RADS v2.1总体特异性较PI-RADS v2有所提高;共5项研究采用阈值4,采用阈值4时PI-RADS v2.1总体敏感度较PI-RADS v2没有明显提高;PI-RADS v2.1较PI-RADS v2总体特异性有所提高。无论是PI-RADS v2还是PI-RADS v2.1,采用阈值3时,总体敏感度均较采用阈值4时稍高,采用阈值4时,总体特异性均较采用阈值3明显提高,见表 3。PI-RADS v2.1结合4为阈值检测csPCa性能的SROC曲线下面积(AUC)最大,见图 4C。
表 3 不同阈值及不同作者国籍PI-RADSv2.1 vs. PI-RADS v2诊断性能的比较(95%CI)Table 3 Diagnostic performance of PI-RADS v2.1 vs. PI-RADS v2 for different thresholds and different nationalities of the authors (95%CI)
2.3.4 不同国籍(中国 vs. 国外)诊断性能亚组分析
纳入的中国研究共5项,中国的研究PI-RADS v2与PI-RADS v2.1的总体敏感度相同;PI-RADS v2的总体特异性较PI-RADS v2.1有所提高;纳入的国外研究共7项,国外的研究PI-RADS v2.1的总体敏感度较PI-RADS v2没有明显提高,PI-RADS v2.1的总体特异性较PI-RADS v2有所提高。中国的研究PI-RADS v2和PI-RADS v2.1总体敏感度和国外的研究相同,总体特异性明显高于国外研究,见表 3。PI-RADS v2.1的中国研究在检测csPCa性能的SROC曲线下面积(AUC)最大,见图 4D。
3 讨论
高危患者在前列腺活检前进行MRI检查,以对其进行风险分层,指导前列腺活检。PI-RADS旨在标准化前列腺MRI的成像参数、术语和报告[18]。PI-RADS v2虽然在临床得到广泛应用,但仍有局限性,如DWI评分模糊、不同研究之间诊断准确性存在差异等[19]。因此,在2019年引入了PI-RADS v2.1,在不改变PI-RADS v2总体目标的情况下,通过微小的修改来改善这些局限性[2]。PI-RADS v2对T2加权成像(T2weightedimaging, T2WI)评分为2分的病变未进行分类,PI-RADS v2.1的一个重要变化是T2WI对TZ评分为2分病变进行分类评估,如果DWI评分≤3分,那么病变总评分为2分,如果DWI评分为≥4,那么病变总评分提升至3分。典型囊变的良性前列腺增生(benign prostatic hyperplasia, BPH)结节T2WI评分为1分,新分类的“非典型结节”T2WI评分为2分。
本研究结果表明,PI-RADS v2.1与PI-RADS v2检测csPCa的敏感度(分别为0.92与0.93)都较高,从v2升级到v2.1版本总体敏感度并没有明显提高,但是在TZ中,敏感度稍微有所提高(0.92与0.93),但提高也并不明显。因此,对于临床怀疑前列腺癌的患者,MRI被推荐作为筛查的一线检查手段[20]。然而其特异性都比较低,尽管PI-RADS v2.1的特异性(0.64)较PI-RADS v2(0.57)有所提高,但总体还是处于中等水平。这可能会影响患者主动监测的长期成本效益,因此MRI靶向活检监测被整合到主动监测方案中,以优化诊断,改善监测期间疾病状态评估[21-22]。PI-RADS v2.1特异性有所提高,可能由于基于DWI序列的非典型结节由2分(PI-RADS v2)升级到了3分。由于DWI序列是肿瘤多参数MR成像的重要序列,有学者建议T2WI评分为3分、且DWI评分 < 4分的TZ病变可降至2分,这可能会提高PI-RADS的特异性。
本研究结果与Lee等[23]学者的研究结果有些不同。Lee的Meta分析显示PI-RADS v2.1比v2的特异性显著降低,该分析纳入了8项研究(本研究纳入了其中7项研究,其中1项研究[4]没有明确指出是关于csPCa的而被排除),并且Lee的研究只纳入了英文文献,本研究纳入了5篇中文文献,并且本研究采用Lee纳入的8项研究进行验证时得出结果与其结果一致,目前结果的差异可能是本研究纳入了更多的研究,导致研究结果异质性增大。本结果与Park等[24]学者的Meta分析结果基本一致。
此外,本研究还对阈值和作者国籍进行了亚组分析。研究发现不管阈值为3还是4,PI-RADS v2.1与v2诊断csPCa的SEN、SPE、PLR、NLR、DOR差异均明显;然而,不管PI-RADS v2.1还是v2在阈值取4时,SPE、PLR、DOR都比阈值取3时有显著提高。在不同国籍的亚组分析中也得到类似的结果,不管中国还是外国,PI-RADS v2.1与v2诊断csPCa的SEN、SPE、PLR、NLR、DOR差异不显著;然而,不管PI-RADS v2.1还是v2在中国研究中,SPE、PLR、DOR都比外国的研究有显著提高。这提示选取不同阈值可能会造成研究异质性,同时中国的研究特异性明显高于国外的,可能与国内学者大多选取阈值为4有关。
本研究尚存在一定局限性:(1)各研究之间存在一定的异质性,但在可接受范围内;(2)不同研究的扫描参数不同可能会影响研究结果一致性;(3)纳入的文献相对较少,但我们已经纳入常见数据库的所有相关文献,纳入的12项研究的总体数量较少,关于PZ区研究少于4项,而未能进行亚组分析;(4)纳入研究均为回顾性研究,这可能会引入发表偏倚。与2015年发布的PI-RADS v2相比,PI-RADS v2.1在2019年刚刚实施,相对较短的经验也可能是研究结果中的混淆因素。
PI-RADS v2.1与PI-RADS v2比较,在诊断性能方面并没有显著提升,总体特异性仍为中等水平,这可能导致阴性活检率增加,特别是对于PI-RADS评分为3分的病变特异性较差,可以考虑通过调整阈值来提高总体诊断的特异性。
Competing interests: The authors declare that they have no competing interests.利益冲突声明:所有作者均声明不存在利益冲突。作者贡献:白国杰:文献检索、数据分析、文献质量评价、论文撰写与修改李珂欣、张克宇:论文设计、文献筛选、论文撰写指导刘文远、孙雅苹、王煜:数据提取、数据整理、数据核对兰广、郭红:制定检索策略、文献检索、文献初筛童卫玲:文献筛选、文献质量评价 -
![]()
图 3 所有分区PI-RADS v2.1与PI-RADS v2诊断性能森林图
Figure 3 Forest maps of diagnostic performance of PI-RADS v2.1 and PI-RADS v2 for all zones
![]()
图 4 PI-RADS v2.1 vs. PI-RADS v2诊断性能SROC曲线
Figure 4 SROC curves of diagnostic performance ofPI-RADSv2.1 vs. PI-RADSv2
表 2 PI-RADS v2.1 vs. PI-RADS v2对整个腺体及移形带csPCa的诊断性能(95%CI)
Table 2 Diagnostic performance of PI-RADS v2.1 vs. PI-RADS v2 for the whole gland and transition zone csPCa (95%CI)
 下载: 导出CSV
下载: 导出CSV
表 3 不同阈值及不同作者国籍PI-RADSv2.1 vs. PI-RADS v2诊断性能的比较(95%CI)
Table 3 Diagnostic performance of PI-RADS v2.1 vs. PI-RADS v2 for different thresholds and different nationalities of the authors (95%CI)
下载: 导出CSV
-
[1] Kasivisvanathan V, Stabile A, Neves JB, et al. Magnetic Resonance Imaging-targeted Biopsy Versus Systematic Biopsyin the Detection of Prostate Cancer: A Systematic Review and Metaanalysis[ J]. Eur Urol, 2019, 76(3): 284-303. doi: 10.1016/j.eururo.2019.04.043
[2] Turkbey B, Rosenkrantz AB, Haider MA, et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Updateof Prostate Imaging Reporting and Data System Version 2[J]. Eur Urol, 2019, 76(3): 340-351. doi: 10.1016/j.eururo.2019.02.033
[3] Linhares Moreira AS, De Visschere P, Van Praet C, et al. How does PI-RADS v2.1 impact patient classification? A head-to-head comparison between PI-RADS v2.0 and v2.1[J]. Acta Radiol, 2021, 62(6): 839-847. doi: 10.1177/0284185120941831
[4] Wang Z, Zhao W, Shen J, et al. PI-RADS version 2.1scoring system is superior in detecting transition zone prostate cancer: adiagnostic study[J]. Abdom Radiol (NY), 2020, 45(12): 4142-4149. doi: 10.1007/s00261-020-02724-y
[5] Oerther B, Engel H, Bamberg F, et al. Cancerdetection rates of the PI-RADSv2.1 assessment categories: systematic review andmetaanalysis on lesion level and patient level[J]. Prostate Cancer Prostatic Dis, 2022, 25(2): 256-263. doi: 10.1038/s41391-021-00417-1
[6] Bhayana R, O'Shea A, Anderson MA, et al. PI-RADS Versions 2 and 2.1: Interobserver Agreementand Diagnostic Performance in Peripheral and Transition Zone Lesions Among Six Radiologists[J]. AJR Am J Roentgenol, 2021, 217(1): 141-151. doi: 10.2214/AJR.20.24199
[7] Byun J, Park KJ, Kim MH, et al. Direct Comparison of PI-RADS Version 2 and2.1 in Transition Zone Lesions for Detection of Prostate Cancer: Preliminary Experience[J]. J Magn Reson Imaging, 2020, 52(2): 577-586. doi: 10.1002/jmri.27080
[8] Hötker AM, Blüthgen C, Rupp NJ, et al. Comparisonof the PIRADS 2.1 scoring system to PI-RADS 2.0: Impact on diagnostic accuracyand inter-reader agreement[J]. PLoS One, 2020, 15(10): e0239975. doi: 10.1371/journal.pone.0239975
[9] Kim HS, Kwon GY, Kim MJ, et al. Prostate Imaging-Reporting and Data System: Comparison of the Diagnostic Performance between Version 2.0 and 2.1 forProstatic Peripheral Zone[J]. Korean J Radiol, 2021, 22(7): 1100-1109. doi: 10.3348/kjr.2020.0837
[10] Kim N, Kim S, Prabhu V, et al. Comparison of Prostate Imaging and Reporting Data SystemV2.0 and V2.1 for Evaluation of Transition Zone Lesions: A 5-Reader 202-Patient Analysis[J]. J Comput Assist Tomogr, 2022, 46(4): 523-529. doi: 10.1097/RCT.0000000000001313
[11] Rudolph MM, Baur ADJ, Cash H, et al. Diagnostic performance of PI-RADS version 2.1 compared to version 2.0 for detection of peripheral and transition zone prostate cancer[J]. Sci Rep, 2020, 10(1): 15982. doi: 10.1038/s41598-020-72544-z
[12] Tamada T, Kido A, Takeuchi M, et al. Comparison of PI-RADS version 2 and PI-RADS version 2.1 for the detection of transition zone prostate cancer[J]. Eur J Radiol, 2019, 121: 108704. doi: 10.1016/j.ejrad.2019.108704
[13] 檀双秀, 张跃跃, 王姗, 等. 第2版和第2.1版前列腺影像报告与数据系统对临床显著性前列腺癌诊断效能的比较分析[J]. 中华放射学杂志, 2021, 55(2): 160-165. doi: 10.3760/cma.j.cn112149-20200212-00144 Tan SX, Zhang YY, Wang S, et al. Comparison of the diagnostic value of prostate imaging reporting and data system version 2 and version 2.1 in the detection of clinically significant prostate cancer[J]. Zhonghua Fang She Xue Za Zhi, 2021, 55(2): 160-165. doi: 10.3760/cma.j.cn112149-20200212-00144
[14] Wei CG, Zhang YY, Pan P, et al. Diagnostic Accuracy and Interobserver Agreement of PI-RADS Version 2 and Version 2.1 for the Detection of Transition Zone Prostate Cancers[J]. AJR Am J Roentgenol, 2021, 216(5): 1247-1256. doi: 10.2214/AJR.20.23883
[15] Xu L, Zhang G, Zhang D, et al. Comparison of PI-RADS version 2.1 and PI-RADS version 2 regardinginterreader variability and diagnostic accuracy for transition zone prostatecancer[J]. Abdom Radiol (NY), 2020, 45(12): 4133-4141. doi: 10.1007/s00261-020-02738-6
[16] 张沥, 李陇超, 张鑫, 等. 前列腺影像报告和数据系统2.1版与2版对前列腺癌的诊断价值比较[J]. 临床放射学杂志, 2020, 39(11): 2262-2266. doi: 10.13437/j.cnki.jcr.2020.11.027 Zhang L, Li LC, Zhang X, et al, Comparison the Diagnostic Value of Prostate Imaging Reporting and Data System Version 2.1 and Version 2[J]. Lin Chuang Fang She Xue Za Zhi, 2020, 39(11): 2262-2266. doi: 10.13437/j.cnki.jcr.2020.11.027
[17] 张丹, 朱子超, 宋娜, 等. PI-RADS v2.1和PI-RADS v2对移行带前列腺癌诊断价值的研究[J]. 磁共振成像, 2022, 13(1): 54-58. https://www.cnki.com.cn/Article/CJFDTOTAL-CGZC202201011.htm Zhang D, Zhu ZC, Song N, et al. Study of PI-RADS v2.1 and PI-RADS v2 for diagnostic value of transition zone prostate cancer[J]. Ci Gong Zhen Cheng Xiang, 2022, 13(1): 54-58. https://www.cnki.com.cn/Article/CJFDTOTAL-CGZC202201011.htm
[18] Weinreb JC, Barentsz JO, Choyke PL, et al. PI-RADS ProstateImaging- Reporting and Data System: 2015, Version 2[J]. Eur Urol, 2016, 69(1): 16-40. doi: 10.1016/j.eururo.2015.08.052
[19] Padhani AR, Weinreb J, Rosenkrantz AB, et al. Prostate Imaging-Reporting and Data System Steering Committee: PI-RADS v2 Status Update and Future Directions[J]. Eur Urol, 2019, 75(3): 385-396. doi: 10.1016/j.eururo.2018.05.035
[20] Mottet N, van den Bergh RCN, Briers E, et al. EAU-EANMESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent[J]. Eur Urol, 2021, 79(2): 243-262. doi: 10.1016/j.eururo.2020.09.042
[21] Ploussard G, Renard-Penna R. MRI-guided active surveillance in prostatecancer: not yet ready for practice[J]. Nat Rev Urol, 2021, 18(2): 77-78. doi: 10.1038/s41585-020-00416-2
[22] Barrett T, Haider MA. The Emerging Role of MRI in Prostate Cancer Active Surveillance and Ongoing Challenges[J]. AJR Am J Roentgenol, 2017, 208(1): 131-139. doi: 10.2214/AJR.16.16355
[23] Lee CH, Vellayappan B, Tan CH. Comparison of diagnostic performance and inter-reader agreement between PI-RADS v2.1 and PI-RADS v2: systematic review and meta-analysis[J]. Br J Radiol, 2022, 95(1131): 20210509. doi: 10.1259/bjr.20210509
[24] Park KJ, Choi SH, Kim MH, et al. Performance of Prostate Imaging Reporting and Data System Version 2.1 for Diagnosis of Prostate Cancer: A Systematic Review and Meta-Analysis[J]. J Magn Reson Imaging, 2021, 54(1): 103-112. doi: 10.1002/jmri.27546
-
期刊类型引用(1)
1. 柯楠,刘凯,陈娇,李晶. 改良PI-RADS评分联合血清AGR2、sTim-3水平对前列腺癌的诊断价值. 中国性科学. 2025(01): 40-44 .  百度学术
百度学术
其他类型引用(1)
计量
- 文章访问数: 1715
- HTML全文浏览量: 446
- PDF下载量: 472
- 被引次数: 2

