
Predictive Value of Immune Inflammation Combined with Liver Function Hematological Indicators for Metastasis of Colorectal Cancer
-
摘要:目的
探讨免疫炎症联合肝脏功能血液学指标对结直肠癌转移的预测价值。
方法回顾性分析133例结直肠癌患者临床资料,根据术后随访24个月的疾病进展情况,将其分为无转移组(n=38)、肝转移组(n=43)和非肝远处转移组(n=52),分析无进展生存期的免疫炎症指标和肝脏功能血液学指标,单因素和多因素Logistic回归分析结直肠癌发生转移的风险因素,构建列线图预测模型。采用受试者工作特征曲线(ROC)和校准曲线验证列线图的准确度,通过决策曲线和临床影响曲线评价列线图的临床预测效能。
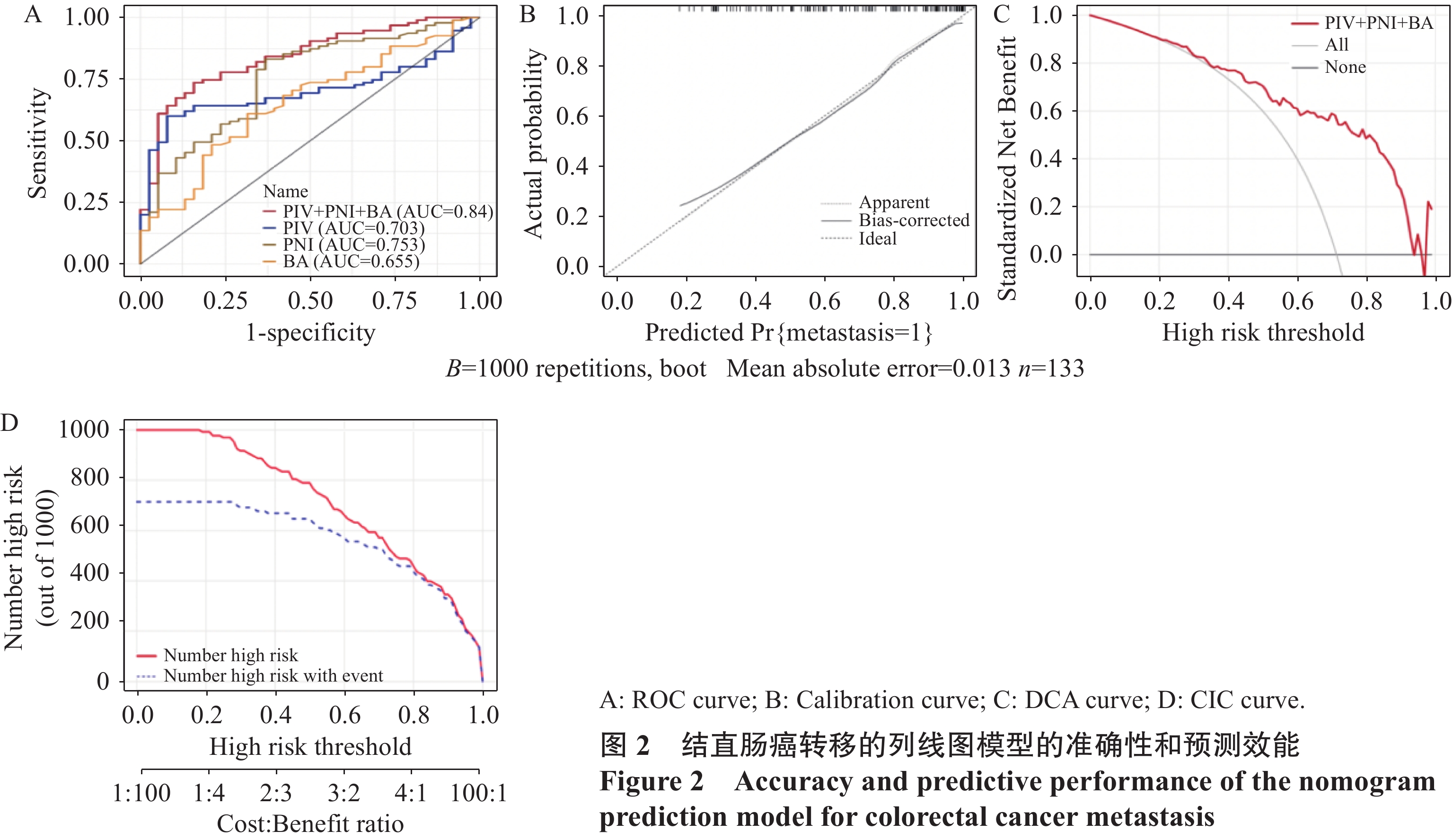
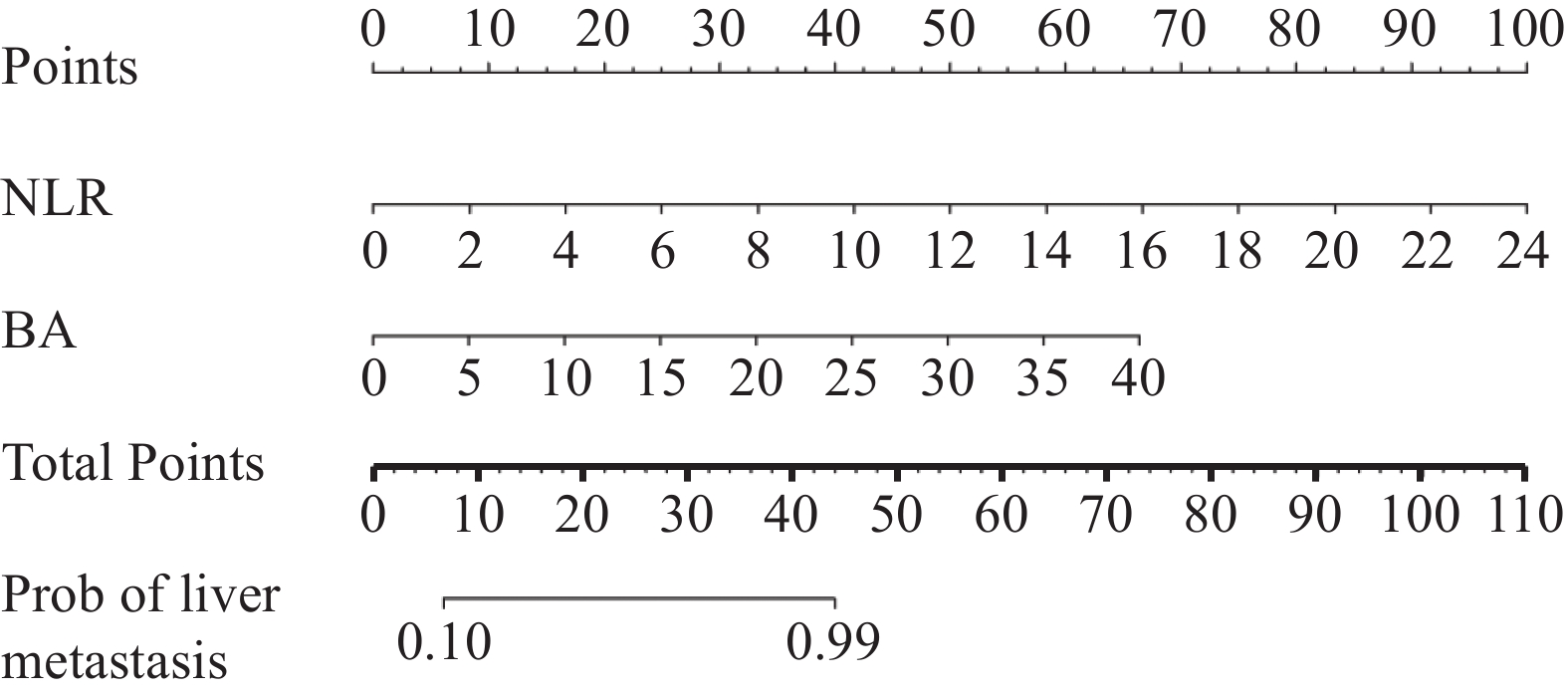
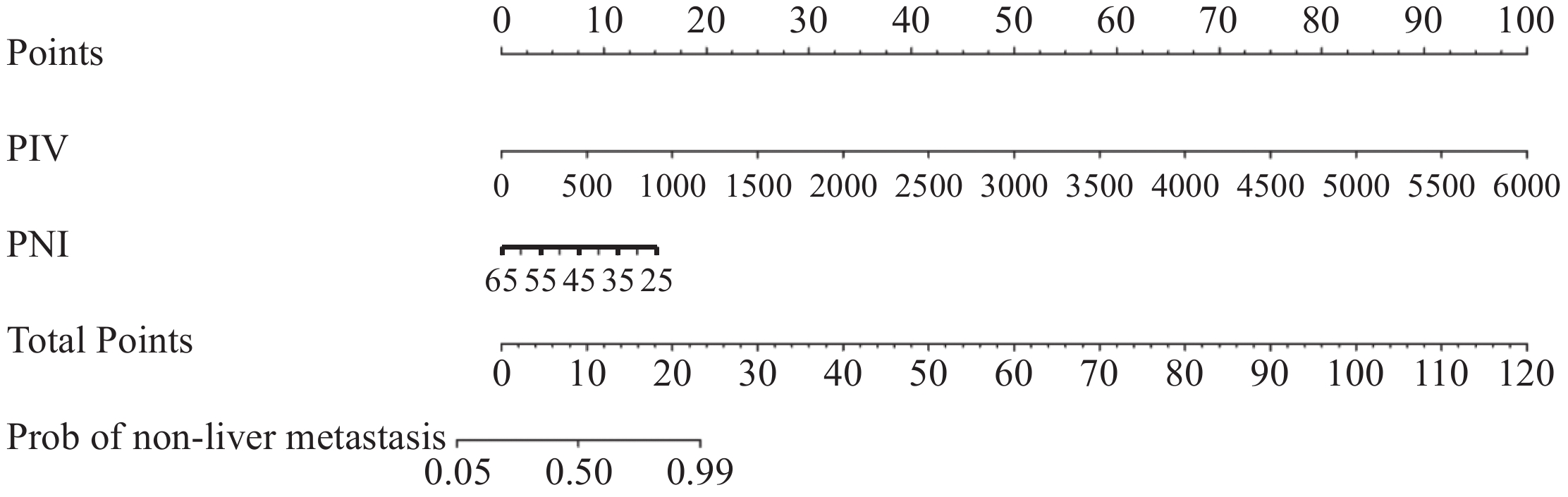
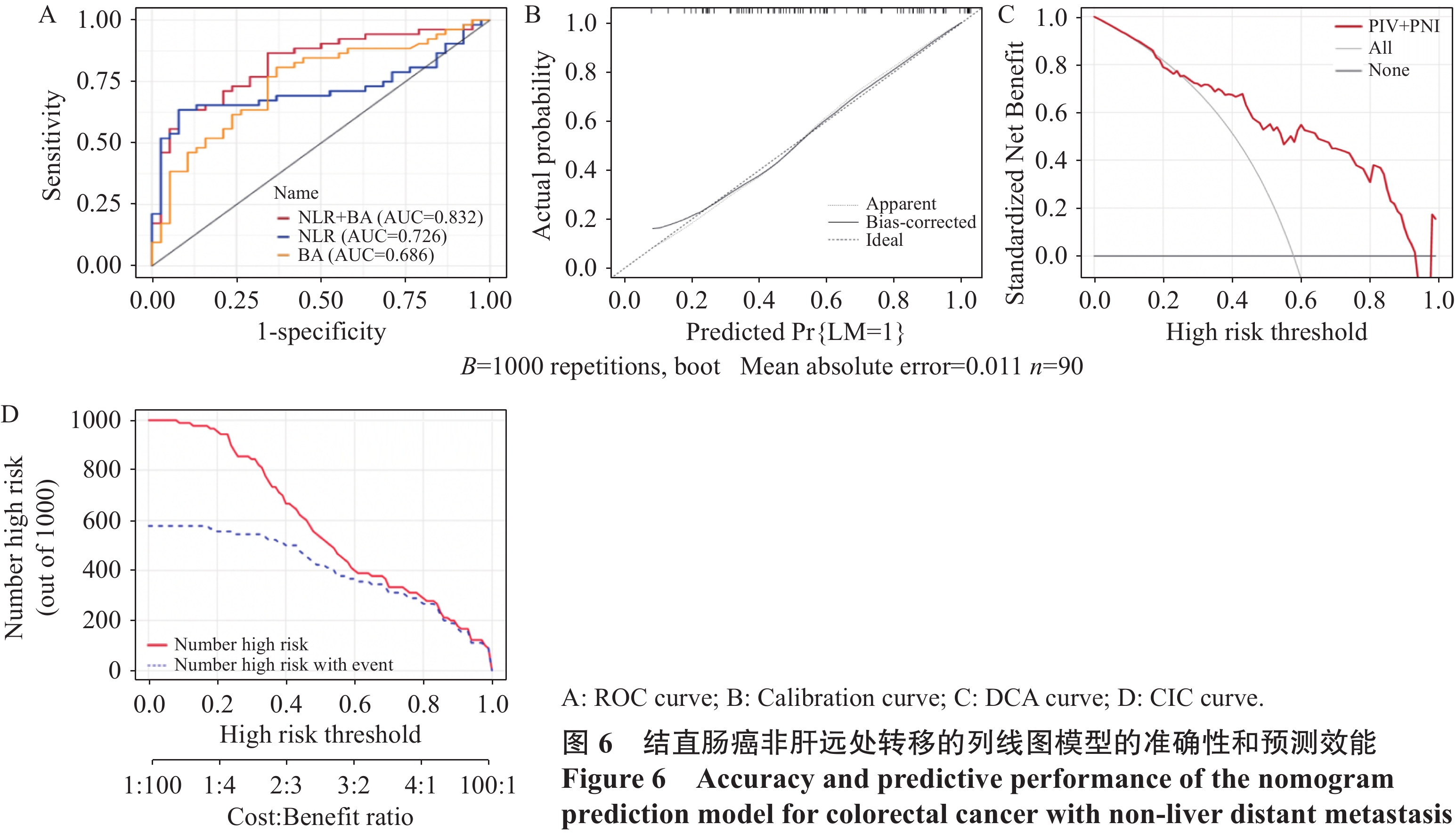
结果单因素及多因素Logistic回归分析显示泛免疫炎症值(PIV)、预后营养指数(PNI)与胆汁酸(BA)是结直肠癌发生转移的独立预测因素,三者联合预测转移的ROC曲线下面积为0.84;中性粒细胞/淋巴细胞比值(NLR)和BA是结直肠癌发生肝转移的独立预测因素,二者联合预测肝转移的ROC曲线下面积为0.83;PIV和PNI是结直肠癌发生非肝远处转移的独立预测因素,二者联合预测非肝远处转移的ROC曲线下面积为0.83;校准曲线、决策曲线和临床影响曲线显示该三种模型具有良好的准确度及净效益值。
结论基于免疫炎症和肝脏功能血液学指标构建的列线图可预测结直肠癌患者的转移情况,具有较高的预测效能及临床应用前景。
Abstract:ObjectiveTo explore the predictive value of immune inflammation combined with liver function hematological indicators for the metastasis of colorectal cancer.
MethodsA retrospective analysis of clinical data of 133 patients with colorectal cancer was conducted. The patients were divided into three groups based on disease progression after 24 months of postoperative follow-up: non-metastasis group (n=38), liver metastasis group (n=43), and non-liver distant metastasis group (n=52). The immune inflammatory markers and liver function hematological indicators of progression-free survival were analyzed. Nomogram prediction models were constructed using univariate and multivariate logistic regression analyses to identify risk factors for metastasis of colorectal cancer. The accuracy of the nomogram was validated using receiver operating characteristic (ROC) curve and calibration curve, and the clinical predictive efficacy was evaluated through decision curve and clinical impact curve.
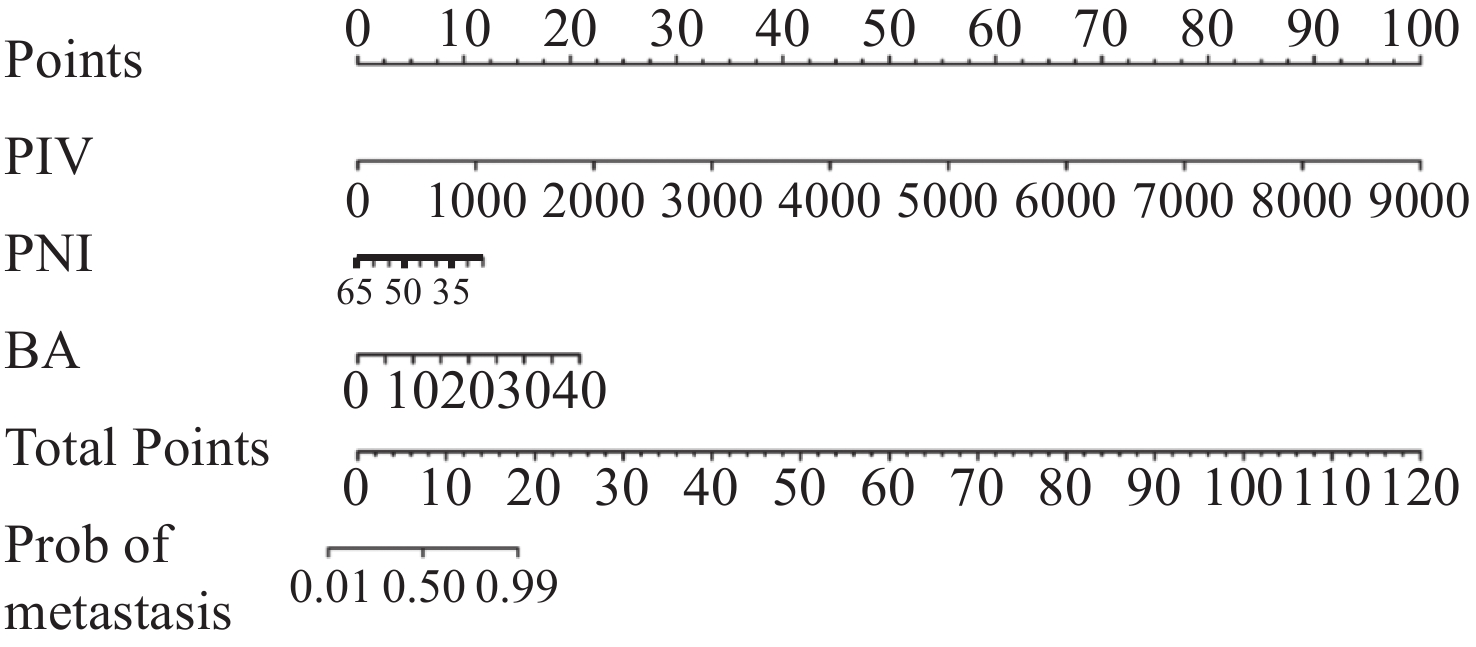
ResultsUnivariate and multivariate logistic regression analyses showed that pan-immune-inflammatory value (PIV), prognostic nutritional index (PNI), and bile acid (BA) were independent predictors of colorectal cancer metastasis. The area under the ROC curve of the combined prediction of metastasis was 0.84; neutrophil/lymphocyte ratio (NLR) and BA were independent predictors of liver metastasis from colorectal cancer. The area under the ROC curve of the combined prediction of liver metastasis was 0.83; PIV and PNI were independent predictive factors for the occurrence of non-liver distant metastasis from colorectal cancer. The area under the ROC curve for the combined prediction of non-liver distant metastasis was 0.83. The calibration curve, decision curve, and clinical impact curve showed that the three models had good accuracy and net benefit value.
ConclusionThe nomogram constructed based on immune inflammation and liver function hematological indicators can predict the metastasis of patients with colorectal cancer and has high predictive efficacy and clinical application prospects.
-
Key words:
- Immune inflammation /
- Liver function /
- Hematological indicators /
- Colorectal cancer /
- Metastasis /
- Predictive value
-
0 引言
中国前列腺癌粗发病率为2.98/10万~17.69/10万,较欧美发达国家低,但在亚洲处于较高发病水平,且在过去10年中总体呈增长趋势[1],城市男性前列腺癌发病率约为农村的3.7倍。70岁以上中国男性的前列腺癌居男性泌尿生殖系肿瘤发病率第一位[2]。在晚期前列腺癌或不适合根治术的患者中,内分泌治疗显得尤为重要,内分泌治疗目前主要包括手术及药物去势、单一抗雄和最大雄激素阻断(maximum androgen blockade, MAB),而内分泌治疗的中位缓解时间为18~24月[3],随后大多数患者会进入去势抵抗阶段,即变成去势抵抗性前列腺癌(castration-resistant prostate cancer, CRPC),只是在相同内分泌治疗前提下进入的时间却有差异。一旦发生CRPC,往往成为临床上诊治的难点。因此急需要找到相关临床指标作为危险或保护因素,早期采取措施,加以预防,尽量延长从治疗确诊到进入CRPC的时间,使患者获益。
1 资料与方法
1.1 诊断标准
根据2014版《中国泌尿外科疾病诊断治疗指南》,CRPC的定义是:经过初次持续雄激素剥夺治疗后疾病依然进展的前列腺癌,且同时具备血清睾酮达到去势水平(小于50 ng/dl或小于1.7 nmol/L)和间隔1周连续3次PSA上升,较最低值升高50%以上两个条件。以第一次升高时间为去势抵抗发生时间。
1.2 纳入标准
(1)穿刺病理符合前列腺癌诊断标准,并且失去手术指征的前列腺癌患者;(2)在确诊前列腺癌后的2年内发生去势抵抗,并符合去势抵抗性前列腺癌的诊断;(3)已采取去势及抗雄治疗(包括手术去势、药物去势或全雄阻断)。
1.3 排除标准
(1)有其他泌尿系统疾病及其他严重心肝肾疾病,包括除前列腺癌外的第二原发肿瘤;(2)已使用化疗(诊断为CRPC后使用除外);(3)未按规定治疗和资料不全者。
1.4 一般资料
从2012年1月至2019年5月,在就诊于广州中医药大学第一附属医院泌尿外科病房及广东省中医院芳村分院泌尿外科病房的前列腺癌患者中,选取符合纳入标准的病例。
1.5 观察指标、研究方法
应用病例-对照研究方法,将进展为去势抵抗性前列腺癌(CRPC)的患者作为病例组,实施1:1配比对照组,配比条件为同种族、同患前列腺癌、同行内分泌治疗(包括手术去势、药物去势或全雄阻断)。回顾性调查相关因素包括:年龄、治疗前PSA、Gleason评分、肿瘤T分期、是否远处转移、是否淋巴结转移、前列腺体积以及内分泌治疗后的“治疗后PSA最低值(PSA nadir)”、“到达最低值时间(TTN)”。
1.6 统计学方法
计量资料用(

2 结果
2.1 一般资料比较
共142例患者纳入研究,其中病例组71例,对照组71例。对照组中2例因数据不齐而脱失,故实际对照组例数为69例,实际总例数140例,平均年龄为73.94±8.17岁,其中确诊前列腺癌最小年龄为49岁,最大为91岁。PSA平均值为418.39±799.08 ng/ml,最小值为6.83 ng/ml,最大值为5 000.00 ng/ml。PSA nadir的平均值为10.28±72.52 ng/ml(0~822.00 ng/ml)。TTN的平均时间为11.20±9.71月(1.8~53月)。前列腺体积平均值为62.81±56.92 cm3(12.17 cm3~371.24 cm3)。
2.2 单因素分析
治疗前PSA、PSA nadir、TTN、肿瘤T分期、淋巴结转移和远处转移均有统计学意义(P < 0.05),年龄、GS评分和前列腺体积均无统计学意义(P > 0.05)。
2.3 多因素分析(二元Logistic回归分析)
纳入模型的变量中,具有显著差异的临床指标有:PSA nadir和TTN(P < 0.05)。根据结果:PSA nadir的β=1.936 > 0,OR=6.930 > 1,表明PSA nadir是CRPC发生的危险因素,PSA nadir越高,2年内进展为CRPC概率越大。TTN的β=-0.215 < 0,OR=0.806 < 1,表明TTN是CRPC发生的保护因素,即TTN时间越长,2年内进展为CRPC的概率越小,见表 1~2。
表 1 模型预测去势抵抗性前列腺癌的准确性Table 1 Accuracy of prediction model of CRPC 表 2 去势抵抗性前列腺癌二元Logistic回归分析Table 2 Logistic regression analysis results of risk factors of CRPC
表 2 去势抵抗性前列腺癌二元Logistic回归分析Table 2 Logistic regression analysis results of risk factors of CRPC
2.4 生存分析
病例组进展为CRPC的平均时间为10.49±5.27月,具体分组作Kaplan-Meier分析如下:以TTN作为分组,TTN的二分类标准目前尚没有公认的分组方法,纪光杰等[4]将TTN以9月为界分为两组,现本研究沿用此依据,将TTN分为≤9月和 > 9月组,以“发生CRPC”作为终点事件,经过Log rank(Mantel-Cox)检验,差异具有统计学意义(P < 0.05),TTN≤9月时,发生CRPC中位时间为8.29月(95%CI: 7.033~9.547);TTN > 9月时,发生CRPC中位时间为16月(95%CI: 13.835~18.165);生存分析见图 1。
以PSA nadir作为分组,分为≤0.2 ng/ml和 > 0.2 ng/ml组[3, 5-6],以“发生CRPC”作为终点事件,经过Log rank(Mantel-Cox)检验,差异具有统计学意义(P < 0.05),PSA nadir≤0.2 ng/ml时,发生CRPC中位时间为12月(95%CI: 9.253~14.747);PSA nadir > 0.2 ng/ml时,发生CRPC中位时间为9月(95%CI: 7.008~10.992)。生存分析见图 2。
![]() 图 2 以PSA nadir分组去势抵抗性前列腺癌的生存分析Figure 2 Survival analysis of CRPC patients according to PSA nadir
图 2 以PSA nadir分组去势抵抗性前列腺癌的生存分析Figure 2 Survival analysis of CRPC patients according to PSA nadir3 讨论
前列腺癌的若干临床因素除了为疾病当前的状态提供诊疗方案外,还可以探讨其预测CRPC作用。针对本研究,以下分述各个临床指标预测CRPC的作用。
3.1 初始PSA
经过多因素综合分析,得出初始PSA高低并非早期进展为CRPC的危险因素。纪光杰等[4]研究亦认为CRPC患者与非CRPC患者在初始PSA的比较上无显著差异,和本课题研究结果一致。
3.2 PSA nadir
本文研究结果表明PSA nadir可能是早期进展为CRPC的独立危险因素。这与纪光杰等[4]及徐凡等[5]研究结果相同,可能与PSA高低能够直接反应内分泌药物的敏感度有关。一般全雄阻断后PSA能够较快下降至低值,若睾酮达到去势水平的情况下,未达到最低值,说明对其药物已失去敏感度,进入CRPC阶段,故PSA nadir可能是CRPC的独立危险因素。临床需密切关注内分泌治疗后患者的PSA波动,关注其最低值情况,以评估早期进展为CRPC的风险,提早做好防治准备。但有学者[7]提出由于PSA nadir的出现是在内分泌治疗一段时间后,并不能较早预测CRPC发生,然而在更换二线内分泌治疗药物时,可根据PSA nadir的高低来选择药物组合。在生存分析方面,徐帆等[5]在COX回归分析中发现PSA nadir≤0.2 ng/ml时,中位CRPC时间为47.6月,PSA nadir > 0.2 ng/ml时,中位CRPC时间仅10.4月,本研究结果与徐帆相似,但数值降低更显著,这可能与本研究纳入标准比较严格有关。目前PSA nadir是否能在结局发生的时间上起作用尚有争议,但可以明确的是,经过Logistic分析,PSA nadir可能是早期进展为CRPC的独立危险因素。
3.3 到达tPSA最低值所需时间(TTN)
从多因素分析可知,TTN属于保护因素。既往已有生存分析研究显示,TTN≤9月组的中位CRPC时间为13.2月,TTN > 9月组为38.4月[5],另一研究显示TTN≤9月组为23月,TTN > 9月组为57月[4]。以上两项研究的多因素分析均与本研究生存分析结果相似,即TTN越小,进展为CRPC时间越短,属于CRPC的保护因素。Teoh等[8]研究发现PSA下降到最低值的时间越快,无进展生存期和总生存期越短。但本研究的两组数据比这两项研究均要短,可能与纳入排除标准的制定、地域因素、治疗差异有关。虽然Teoh等研究的终点事件是死亡事件的发生,但结合本研究,也能说明TTN可作为保护因素,预测前列腺癌及CRPC的预后,即TTN越长,下降到最低值的时间越慢,越能延迟CRPC的发生。探其原因,主要有以下两点:第一,Thomas等[9]研究化疗的CRPC患者中认为过快地杀死化疗敏感性前列腺癌细胞有可能为化疗耐受性前列腺癌细胞提供更有利的生存环境。同理,我们推断过快杀死激素敏感性前列腺癌细胞,可能为激素非依赖性前列腺癌细胞提供更有利的生存环境,此推断有待大量基础实验证明;第二,有研究显示[10]激素治疗后,PSA有一段过快下降时间,这段时间并不是肿瘤抑制效应,而是雄激素(androgen receptor, AR)通路被抑制而引起的化学效应,这段时期过后,如果PSA继续缓慢下降,则认为是肿瘤负荷减少的反应。
3.4 肿瘤T分期及Gleason评分
初诊前列腺癌即属于局部晚期(T4)的患者在各期中比例最高,这说明很多患者到达一定年纪后不会主动监测PSA,直到有症状出现,而症状的出现亦预示着疾病到达中晚期。一般来说,年龄大于50岁,前列腺癌的发病率升高,因此有必要在50岁时进行PSA监测。TNM分期在CRPC组与非CRPC组在单因素分析上均有意义,但在多因素分析时,TNM分期无显著统计学意义,表明TNM分期并不是早期进展CRPC的危险因素。Gleason评分在单因素分析中无统计学意义,经回顾文献,TNM分期及Gleason两项临床指标在CRPC进展的相关研究中,结果不一。王镇伟[7]研究显示T分期及Gleason评分越高,越早进入CRPC。Benaim等[11]回顾性研究150例接受ADT治疗的前列腺癌患者,发现Gleason < 8分的患者具有更长的无进展生存时间,Gleason评分每增加1分,雄激素剥夺治疗后进展为去势抵抗性前列腺癌的风险将增加70%。但孙涛[6]认为单因素分析中Gleason评分与内分泌治疗敏感时间有相关性,在多因素中却失去了意义,表示Gleason评分在该研究中并不是前列腺癌内分泌治疗敏感时间的独立预后因子。纪光杰等[4]研究显示,单因素分析中TNM分期与Gleason评分与CRPC早期进展与否显著相关,但多因素分析无显著关系。本研究与纪光杰及孙涛研究结果相似,与王镇伟及Benaim研究结果相反,这可能与研究设计、样本量等因素有关,目前暂无可靠数据支撑,TNM分期与Gleason评分在CRPC早期进展的影响尚有待进一步考证。
3.5 前列腺体积
单因素分析中,两组前列腺体积在CRPC早期进展上无统计学意义,这与纪光杰、徐凡等研究一致。说明前列腺体积的大小不能反映后续进展CRPC的快慢,但前列腺体积却是其他前列腺癌并发症的危险因素,郑路[12]研究显示列腺体积是前列腺癌发生骨转移的主要独立危险因素。此外前列腺体积对前列腺癌的诊断有一定影响,欧汝彪等[13]研究认为前列腺体积≤50 ml时,检测PSA、PSAD值对前列腺癌的筛选有重要意义,但前列腺体积 > 50 ml会对PSA、PSAD值形成干扰,导致诊断不明确。虽然本研究提示前列腺体积并不是CRPC的危险因素,但其在CRPC的发生发展中潜在的影响还需进一步发掘与研究。
综上,TTN可能是早期进展为CRPC的保护因素,TTN越长,2年内进展为CRPC的机会越小。PSA nadir可能是早期进展为CRPC的独立危险因素,PSA nadir越高,风险越大。TTN≤9月、PSA nadir > 0.2 ng/ml是CRPC的危险因素。目前CRPC的治疗效果不算理想,主要治疗药物有阿比特龙、阿帕他胺等,治疗手段有限、过程棘手,因此防范于未然的研究可以作为突破点。但本论文属于回顾性分析,证据强度有限,结论只能说明是可能保护因素及可能危险因素,若要找到明确的关系,尚需要大样本相关队列及前瞻性研究证明。
Competing interests: The authors declare that they have no competing interests.利益冲突声明:所有作者均声明不存在利益冲突。作者贡献:褚雪镭:研究分析和撰写论文安宸、席玲泽、谢虹亭、宗铭桐:数据整理薛 鹏:数据校对朱世杰:研究设计和资金支持 -
![]()
图 1 结直肠癌转移的列线图预测模型
Figure 1 Nomogram prediction model for colorectal cancer metastasis
![]()
图 3 结直肠癌肝转移的列线图预测模型
Figure 3 Nomogram prediction model for colorectal cancer liver metastasis
![]()
图 5 结直肠癌非肝远处转移的列线图预测模型
Figure 5 Nomogram prediction model for colorectal cancer with non-liver distant metastasis
表 1 结直肠癌无转移组、肝转移组、非肝远处转移组的一般资料比较
Table 1 Comparison of general data among the non-metastasis group, liver metastasis group, and non-liver distant metastasis group of patients with colorectal cancer
Factors NM group(n=38) LM group(n=43) NLM group(n=52) χ2/F P Age($ \bar{x} $± s, years) 65.55 ± 7.89 65.35 ± 12.22 66.77 ± 10.51 1.178 0.555 Gender(male/female, n) 26/12 28/15 28/24 2.295 0.317 Hypertension(yes/no, n) 19/19 17/26 22/30 0.957 0.620 Hyperglycemia(yes/no, n) 10/28 14/29 13/39 0.729 0.694 Drinking(yes/no, n) 14/24 12/31 16/36 0.771 0.680 Smoking(yes/no, n) 14/24 14/29 19/33 0.216 0.898 Position(colon/rectum, n) 20/18 25/18 28/24 0.285 0.867 BMI($ \bar{x} $± s, kg/m2) 23.57 ± 3.05 22.49 ± 3.72 22.82 ± 3.93 0.934 0.396 Notes: NM: Non-metastasis; LM: Liver metastasis; NLM: Non-liver distant metastasis.  下载: 导出CSV
下载: 导出CSV
表 2 结直肠癌无转移组、肝转移组、非肝远处转移组的血液学资料比较
Table 2 Comparison of hematological data among the non-metastasis group, liver metastasis group, and non-liver distant metastasis group of patients with colorectal cancer
Factors NM group(n=38) LM group(n=43) NLM group(n=52) χ2/F P NEUT 3.00(1.11) 3.88(2.94) 4.26(2.92) 10.592 0.005 LYM 1.52(0.77) 1.10(1.06) 1.34(0.52) 7.058 0.029 MONO 0.33±0.11 0.43±0.26 0.45±0.22 5.687 0.058 PLT 175.00(51.00) 201.00(113.00) 208.00(144.50) 3.834 0.147 ALB 42.52±4.03 37.93±5.33 38.10±5.73 10.303 <0.001 ALT 16.40(13.43) 16.90(11.70) 12.20(10.05) 12.274 0.002 AST 17.40(10.88) 24.80(27.70) 17.10(11.73) 14.329 0.001 BA 2.67(2.69) 5.46(7.55) 3.48(2.86) 10.680 0.005 TC 4.27±0.92 4.44±1.37 4.44±1.02 0.330 0.719 HDL-C 1.13(0.35) 1.18(0.49) 1.07(0.43) 2.309 0.315 LDL-C 2.77±0.87 3.02±1.32 3.00±0.98 0.653 0.522 ApoB 0.91(0.44) 0.98(0.34) 0.98(0.44) 2.121 0.346 ApoA1 1.35(0.25) 1.21(0.44) 1.16(0.31) 15.882 <0.001 CEA 2.60(2.04) 40.12(126.65) 15.42(113.48) 48.968 <0.001 NLR 2.01(1.22) 3.33(3.65) 3.17(3.50) 17.222 <0.001 MLR 0.21(0.13) 0.29(0.38) 0.32(0.21) 12.162 0.002 PLR 124.93(61.67) 154.78(161.30) 157.96(150.78) 11.637 0.003 SII 352.76(197.03) 585.66(851.08) 739.99(966.08) 17.152 <0.001 PIV 123.26(84.58) 229.32(384.18) 299.03(520.59) 13.683 0.001 PNI 51.25(8.56) 45.97(11.10) 45.09(8.85) 20.665 <0.001 ALRI 12.88(10.31) 19.49(38.61) 13.27(16.90) 12.613 0.002 APRI 0.10(0.06) 0.14(0.11) 0.08(0.08) 15.064 0.001
下载: 导出CSV
表 3 结直肠癌术后转移影响因素的单因素分析
Table 3 Univariate analysis of factors influencing postoperative metastasis of colorectal cancer
Factors NM group(n=38) M group(n=95) HR(95%CI) t/z P PIV 123.26(84.58) 261.63(401.42) 0.995(0.992-0.998) −3.651 0.003 PNI 50.51±5.76 44.53±6.73 1.167(1.084-1.255) −4.811 <0.001 ALRI 12.88(10.31) 15.28(17.34) 0.957(0.920-0.995) −2.107 0.027 BA 2.67(2.69) 4.15(4.60) 0.802(0.678-0.947) −2.782 0.010 TC 4.27±0.92 4.44±1.19 0.864(0.609-1.226) 0.816 0.414 ApoB 0.91(0.44) 0.98(0.40) 0.328(0.093-1.155) −1.455 0.083 ApoA1 1.36±1.19 1.16±0.28 26.080(4.385-155.107) −4.708 <0.001 Note: M group: metastasis group.
下载: 导出CSV
表 4 结直肠癌术后转移影响因素的多因素分析
Table 4 Multivariate analysis of factors influencing postoperative metastasis of colorectal cancer
Factors β SE Wald χ2 P OR 95%CI PIV −0.004 0.002 6.246 0.012 0.996 0.992-0.999 PNI 0.105 0.047 5.037 0.025 1.110 1.013-1.216 ALRI −0.015 0.024 0.374 0.541 0.985 0.940-1.033 BA −0.216 0.099 4.795 0.029 0.806 0.664-0.978 ApoA1 0.861 1.117 0.595 0.440 2.366 0.265-21.112 Constant −4.964 2.665 3.470 0.062 0.007 —
下载: 导出CSV
表 5 结直肠癌患者术后肝转移较无转移影响因素的多因素分析
Table 5 Multivariate analysis of factors influencing postoperative liver metastasis compared with non-metastasis in colorectal cancer patients
Factors β SE Wald χ2 P OR 95%CI NLR −0.538 0.257 4.389 0.036 0.584 0.353-0.966 PNI 0.096 0.058 2.709 0.100 1.101 0.982-1.234 BA −0.292 0.103 7.967 0.005 0.747 0.610-0.915 Constant −1.833 3.198 0.328 0.567 0.160
下载: 导出CSV
表 6 结直肠癌患者术后非肝远处转移较无转移影响因素的多因素分析
Table 6 Multivariate analysis of factors influencing non-hepatic distant metastasis compared with non-metastasis in colorectal cancer patient after surgery
Factors β SE Wald χ2 P OR 95%CI PIV 0.005 0.002 6.535 0.011 1.005 1.001-1.009 PNI −0.107 0.047 5.230 0.022 0.898 0.820-0.985 ApoA1 −1.106 1.189 0.866 0.352 0.331 0.032-3.400 constant 5.800 2.380 5.940 0.015 330.350 —
下载: 导出CSV
-
[1] Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2024, 74(3): 229-263. doi: 10.3322/caac.21834
[2] Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022[J]. J Natl Cancer Cent, 2024, 4(1): 47-53. doi: 10.1016/j.jncc.2024.01.006
[3] Chaffer C L, Weinberg R A. A perspective on cancer cell metastasis[J]. Science, 2011, 331(6024): 1559-1564. doi: 10.1126/science.1203543
[4] Hernandez-Alejandro R, Ruffolo L I, Sasaki K, et al. Recipient and Donor Outcomes After Living-Donor Liver Transplant for Unresectable Colorectal Liver Metastases[J]. JAMA Surg, 2022, 157(6): 524-530. doi: 10.1001/jamasurg.2022.0300
[5] Masi G, Vasile E, Loupakis F, et al. Randomized trial of two induction chemotherapy regimens in metastatic colorectal cancer: an updated analysis[J]. J Natl Cancer Inst, 2011, 103(1): 21-30. doi: 10.1093/jnci/djq456
[6] 苏阜力, 张补文. 血清酶活性联检在肝病中的应用[J]. 实用医技杂志, 2006, 13(14): 2435-2436. [Su FL, Zhang BW. Application of combined detection of serum enzyme activity in liver disease[J]. Shi Yong Yi Ji Za Zhi, 2006, 13(14): 2435-2436.] doi: 10.3969/j.issn.1671-5098.2006.14.043 Su FL, Zhang BW. Application of combined detection of serum enzyme activity in liver disease[J]. Shi Yong Yi Ji Za Zhi, 2006, 13(14): 2435-2436. doi: 10.3969/j.issn.1671-5098.2006.14.043
[7] Tian S, Chu Y, Hu J, et al. Tumour-associated neutrophils secrete AGR2 to promote colorectal cancer metastasis via its receptor CD98hc-xCT[J]. Gut, 2022, 71(12): 2489-2501. doi: 10.1136/gutjnl-2021-325137
[8] Khan U, Chowdhury S, Billah MM, et al. Neutrophil Extracellular Traps in Colorectal Cancer Progression and Metastasis[J]. Int J Mol Sci, 2021, 22(14): 7260. doi: 10.3390/ijms22147260
[9] Wang H, Zhang B, Li R, et al. KIAA1199 drives immune suppression to promote colorectal cancer liver metastasis by modulating neutrophil infiltration[J]. Hepatology, 2022, 76(4): 967-981. doi: 10.1002/hep.32383
[10] Lin N, Li J, Yao X, et al. Prognostic value of neutrophil-to-lymphocyte ratio in colorectal cancer liver metastasis: A meta-analysis of results from multivariate analysis[J]. Int J Surg, 2022, 107: 106959. doi: 10.1016/j.ijsu.2022.106959
[11] Tang H, Li B, Zhang A, et al. Prognostic Significance of Neutrophil-to-Lymphocyte Ratio in Colorectal Liver Metastasis: A Systematic Review and Meta-Analysis[J]. PLoS One, 2016, 11(7): e0159447. doi: 10.1371/journal.pone.0159447
[12] Kim H, Jung HI, Kwon SH, et al. Preoperative neutrophil-lymphocyte ratio and CEA is associated with poor prognosis in patients with synchronous colorectal cancer liver metastasis[J]. Ann Surg Treat Res, 2019, 96(4): 191-200. doi: 10.4174/astr.2019.96.4.191
[13] Shibutani M, Maeda K, Nagahara H, et al. The peripheral monocyte count is associated with the density of tumor-associated macrophages in the tumor microenvironment of colorectal cancer: a retrospective study[J]. BMC Cancer, 2017, 17(1): 404. doi: 10.1186/s12885-017-3395-1
[14] Shaul ME, Fridlender ZG. Tumour-associated neutrophils in patients with cancer[J]. Nat Rev Clin Oncol, 2019, 16(10): 601-620. doi: 10.1038/s41571-019-0222-4
[15] Kassassir H, Papiewska-Pająk I, Kryczka J, et al. Platelet-derived microparticles stimulate the invasiveness of colorectal cancer cells via the p38MAPK-MMP-2/MMP-9 axis[J]. Cell Commun Signal, 2023, 21(1): 51. doi: 10.1186/s12964-023-01066-8
[16] Fucà G, Guarini V, Antoniotti C, et al. The Pan-Immune-Inflammation Value is a new prognostic biomarker in metastatic colorectal cancer: results from a pooled-analysis of the Valentino and TRIBE first-line trials[J]. Br J Cancer, 2020, 123(3): 403-409. doi: 10.1038/s41416-020-0894-7
[17] Yang XC, Liu H, Liu DC, et al. Prognostic value of pan-immune-inflammation value in colorectal cancer patients: A systematic review and meta-analysis[J]. Front Oncol, 2022, 12: 1036890. doi: 10.3389/fonc.2022.1036890
[18] Argilés JM, Busquets S, Stemmler B, et al. Cancer cachexia: understanding the molecular basis[J]. Nat Rev Cancer, 2014, 14(11): 754-762. doi: 10.1038/nrc3829
[19] Almasaudi AS, Dolan RD, Edwards CA, et al. Hypoalbuminemia Reflects Nutritional Risk, Body Composition and Systemic Inflammation and Is Independently Associated with Survival in Patients with Colorectal Cancer[J]. Cancers (Basel), 2020, 12(7): 1986. doi: 10.3390/cancers12071986
[20] Hu Z, Li Y, Mao W, et al. Impact of Nutritional Indices on the Survival Outcomes of Patients with Colorectal Cancer[J]. Cancer Manag Res, 2020, 12: 2279-2289. doi: 10.2147/CMAR.S243172
[21] Jung SH, Hao J, Shivakumar M, et al. Development and validation of a novel strong prognostic index for colon cancer through a robust combination of laboratory features for systemic inflammation: a prognostic immune nutritional index[J]. Br J Cancer, 2022, 126(11): 1539-1547. doi: 10.1038/s41416-022-01767-w
[22] Bian X, Liu R, Meng Y, et al. Lipid metabolism and cancer[J]. J Exp Med, 2021, 218(1): e20201606. doi: 10.1084/jem.20201606
[23] Zhang KL, Zhu WW, Wang SH, et al. Organ-specific cholesterol metabolic aberration fuels liver metastasis of colorectal cancer[J]. Theranostics, 2021, 11(13): 6560-6572. doi: 10.7150/thno.55609
[24] Kühn T, Stepien M, López-Nogueroles M, et al. Prediagnostic Plasma Bile Acid Levels and Colon Cancer Risk: A Prospective Study[J]. J Natl Cancer Inst, 2020, 112(5): 516-524. doi: 10.1093/jnci/djz166
[25] Zheng Z, Wei J, Hou X, et al. A High Hepatic Uptake of Conjugated Bile Acids Promotes Colorectal Cancer-Associated Liver Metastasis[J]. Cells, 2022, 11(23): 3810. doi: 10.3390/cells11233810
[26] Thomas DS, Fourkala EO, Apostolidou S, et al. Evaluation of serum CEA, CYFRA21-1 and CA125 for the early detection of colorectal cancer using longitudinal preclinical samples[J]. Br J Cancer, 2015, 113(2): 268-274. doi: 10.1038/bjc.2015.202
[27] Pakdel A, Malekzadeh M, Naghibalhossaini F. The association between preoperative serum CEA concentrations and synchronous liver metastasis in colorectal cancer patients[J]. Cancer Biomark, 2016, 16(2): 245-252. doi: 10.3233/CBM-150561
[28] Lee JH, Lee SW. The Roles of Carcinoembryonic Antigen in Liver Metastasis and Therapeutic Approaches[J]. Gastroenterol Res Pract, 2017, 2017: 7521987.
-
期刊类型引用(4)
1. 郭姗琦,孙彬栩,姜行康,杨同,贾英杰,孔凡铭. 健脾利湿化瘀方联合内分泌治疗对转移性激素敏感性前列腺癌的治疗效果. 肿瘤研究与临床. 2024(07): 503-508 .  百度学术
百度学术
2. 刘和洋,刘倩,红华,金殿生,高慧敏,包森林,李文. 超声影像组学联合模型预测前列腺癌内分泌治疗无进展生存期的价值. 中华超声影像学杂志. 2024(11): 992-999 . 百度学术
3. 张涛,王斌,刘一鸿,席国旺,李中学. 微创经尿道前列腺等离子电切术联合去势治疗高龄晚期前列腺癌的临床研究. 青岛医药卫生. 2023(01): 49-52 . 百度学术
4. 温雪丽. 骨标志物和PSA对前列腺癌发展为CRPC的预测价值. 国际检验医学杂志. 2021(24): 3036-3040 . 百度学术
其他类型引用(8)



计量
- 文章访问数: 1859
- HTML全文浏览量: 2068
- PDF下载量: 687
- 被引次数: 12

