 2015, Vol. 42
2015, Vol. 42文章信息
- 于慧会,魏立璇,刘运泳,邢晓静. 2015
- YU Huihui, WEI Lixuan, LIU Yunyong, XING Xiaojing. 2015
- 25-羟基维生素D与结直肠癌关系的Meta分析
- Meta-analysis of Relationship Between Blood 25-hydroxyvitamin D Level and Colorectal Cancer
- 肿瘤防治研究, 2015, 42(04): 394-398
- Cancer Research on Prevention and Treatment, 2015, 42(04): 394-398
- http://www.zlfzyj.com/CN/10.3971/j.issn.1000-8578.2015.04.017
-
文章历史
- 收稿日期:2014-03-19
- 修回日期:2014-10-14
引用本文 |



2. 110042 沈阳,辽宁省肿瘤防治办公室
2. Liaoning Provincial Cancer Prevention and Treatment Office, Shenyang 110042, China
结直肠癌是目前世界上第三大最常见的恶性肿瘤,全球范围内每年新诊断的结直肠癌病例超过1 200万,并且每年大约有60万人死于这种恶性肿瘤。我国结直肠癌的发病率和死亡率近几年一直呈上升趋势,结直肠癌在恶性肿瘤发病和死亡构成中分别占10.56%和7.80%,居第三位和第五位[1]。
1980年,Garland提出假设,缺乏维生素D的结肠癌患者群中可能具有更高的死亡率[2]。近年来,一些基础研究发现维生素D通过提高细胞分化和凋亡,减少增殖、侵袭、转移潜能和血管新生降低癌症的危险性[3],流行病学研究也在探讨维生素D{其血液中检测指标为25-羟基维生素D[25-hydroxyvitamin D,25-(OH)D]}与结直肠癌的关系[4, 5],然而,25-羟基维生素D水平与结直肠癌的关系仍未定论。本研究采用Meta分析对25-(OH)D水平与结直肠癌关系的前瞻性研究文献进行综合定量分析。1 资料与方法1.1 检索策略
以维生素D、25-羟基维生素D、结直肠癌、结肠癌、直肠癌、大肠癌为中文检索词,以vitamin D、25-(OH)D、colorectal cancer、colon cancer、 r ectal ca n cer为英文检索词。检索数据库包括MEDLINE、EMBASE外文数据库,中国生物医学文献数据库(CBM)、维普数据库、中国知网和万方等中文数据库,并对相关学术会议、报刊文献和未发表的文献等进行相应的检索。检索日期为2003年1月至2013年5月。为防止有被检索策略遗落的文献,对相关文献的参考文献进行手工检索。1.2 文献纳入标准
为提高系统综述水平,本研究写作过程参照系统综述和荟萃分析优先报告的条目:PRISMA声明[6]。文献纳入标准为:(1)文献的研究类型为前瞻性研究。(2)病例为结直肠癌、结肠癌或者直肠癌。(3)文献报道25-(OH)D的水平。对于重复发表的文献,最近的或最大样本量的或原始资料最全的研究将被纳入到本次荟萃分析中。研究对象限制为人体研究。1.3 数据提取
由2名评价员独立提取资料,而后交叉核对,如遇分歧通过讨论解决或由第3位研究者协助解决。资料收集内容主要包括:第一作者姓名、发表时间、研究人群的年龄、国家、研究样本量、随访时间,必要时联系原文献作者,确定试验的具体实施过程。纳入的文献采用文献质量评价标准(Newcastle-Ottawa Scale,NOS)[7]。1.4 统计学方法
数据的综合、归纳和评估应用Stata13.0统计学软件进行分析。1.4.1 异质性分析
采用Q检验判断各研究间是否存在异质性(P<0.05,存在异质性)[8],异质性程度用I2(OR值变异对异质性的贡献)进行评价[9]。若各文献间无异质性用固定效应模型(Mantel-Haenszel方法)计算。反之用随机效应模型(DerSimonianLaird方法)计算。效应量采用RR及其95%置信区间(confidence interval,CI)描述,检验水平α=0.05。1.4.2 发表偏倚
对发表偏倚采用Egger试验和Begg漏斗图评价[10]。2 结果2.1 文献检索
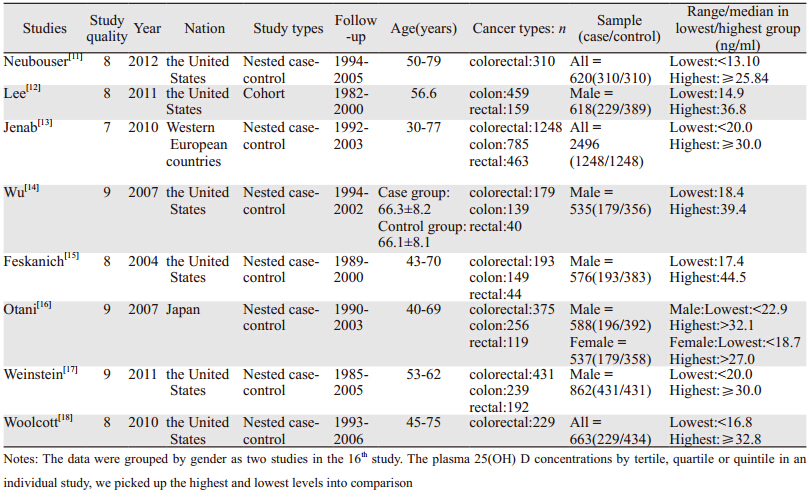
通过文献摘要并对部分文献全文阅读,最终选择8篇进行Meta分析,见图 1。8篇文献均可提取出血液25-(OH)D水平最高组值、最低组值及其他相关信息,见表 1。
 |
| 图 1 文献筛选流程及纳入情况 Figure 1 Flow chart of the studies selection process |
通过提取各纳入文献多因素调整后的RR值,应用Stata13.0软件进行异质性检验(P=0.786,I2=0%),表明纳入的9项研究同质,采用固定效应模型分析。结果表明合并后的结直肠癌血液25-(OH)D水平最高组与最低组比较RR值为0.79(95%CI: 0.65~0.95),可信区间不包含1,说明结直肠癌与血液25-(OH)D升高之间的联系差异有统计学意义,见图 2。
 |
| 图 2 25-(OH)D水平与结直肠癌在不同地区间的关系 Figure 2 Forest plot of 25-(OH)D levels associated with colorectal cancer stratified by region |
按纳入文献中研究对象所在的地理位置将文献分为北美组、欧洲组和东亚组。文献分别为6篇、1篇、1篇。各洲组内不存在统计学异质性。东亚组分析结果显示,结直肠癌患者血液25-(OH)D水平最高组与最低组比较,北美组RR值为0.78(95%CI: 0.60~1.02),欧洲组RR值为0.77(95%CI: 0.56~1.06),东亚组RR值为0.89(95%CI: 0.52~1.50),见图 2。按不同发病部位分为结肠癌组与直肠癌组,RR值和95%CI分别是0.91(0.63~1.33)、0.60(0.31~1.15),表明维生素D与直肠癌的关系较结肠癌的更紧密,见图 3。
 |
| 图 3 25-(OH)D水平与结直肠癌在不同发病部位间的关系Figure 3 Forest plot of 25-(OH)D levels associated with colorectal cancer stratified different pathogenic sites |
Egger’s检验显示整个研究中无明显发表偏倚(P=0.40)。由Begg’s漏斗图可见,漏斗图基本对称,表明无明显发表偏倚,见图 4。
 |
| 图 4 检验纳入文献是否存在发表偏倚的漏斗图 Figure 4 Funnel plot of included studies with or without publication bias |
本研究中共纳入8篇文献,均为前瞻性的观察性研究,其中7篇为前瞻性巢式病例对照研究,1篇为队列研究,总病例数为3 194例,对照数为4 301例。研究显示血液中较低的25-(OH)D水平与结直肠癌的危险性存在一定的联系。在各洲组的分析显示血液中25-(OH)D水平与结直肠癌联系无统计学意义,在结肠癌与直肠癌的亚组分析中血液中25-(OH)D水平与结直肠癌联系无统计学意义。
不同组织的细胞能将25-(OH)D转化成1,25-(OH)2D,进而激活维生素D受体,从而影响多种转录变化。如果25-(OH)D水平较低,不足以维持1,25-(OH)2D的生理浓度,将导致包括分化、增殖、侵袭、血管生成和转移潜能途径的畸变。因此,血液中25-(OH)D含量长期不足,可增加发生癌症的危险性。Trivedi等[19]关于2 686名65~85岁的英国人的随机对照试验(试验组每天服用820IU维生素D,对照组使用安慰剂),经过5年的随访发现,试验组血液25-(OH)D水平为29.7 ng/ml,安慰剂组为21.7 ng/ml,两组间的结直肠癌发病率差异无统计学意义(HR=1.02,95%CI=0.60~1.74)。其原因可能是因为研究样本量较少,随访时间较短。Edward Giovannucci[20]教授综合分析了观察性研究和随机对照试验,建议应保持血液25-(OH)D水平在30~40 ng/ml,这一建议与一份内分泌协会的临床实践指南[21]是一致的。
一些研究报道[22, 23],结肠癌和直肠癌的病因存在差异,维生素D受体的多态性在两者之间同样存在差异。有研究表明维生素D与直肠癌的关系要强于与结肠癌的关系[24],本研究虽然显示直肠癌组合并后的效应值小于结肠癌组的,但由于可信区间包含1,故不能支持Huncharek等[24]研究结果。
本Meta分析纳入文献的平均随访时间超过10年,样本量较大。同时,以往有关二分类资料 Meta分析,主要是通过试验组发生事件(如死亡)数、未发生事件(如未死亡)数、对照组发生事件(如死亡)数和未发生事件(如未死亡)数四个变量进行合并分析。本研究使用了原始文献中经过校正的效应值(RR)和可信区间(95%CI)进行Meta分析,排除了一些混杂因素的影响,使研究结果更可信。文献是否查全是影响Meta分析结果的一个重要因素,为了解决这个问题,本研究制定了严格的检索策略,并对不同的数据库进行重复检索,并由专人进行审查核对,最大程度上减少了因文献检索所造成的偏倚。
本研究存在一定的局限性,在亚组分析中,有的组别因为所纳入文献较少,如欧洲组只纳入一个文献,可能增加了研究结果的不确定性。东亚组的两组数据,实为同一篇文章的男性数据和女性数据,样本量相对较少。
总之,本Me ta分析发现血液中较低的25 -(OH)D水平与结直肠癌发生存在联系,但目前有关25-(OH)D水平与结直肠癌关系的文献可利用数据不多,而且未有以中国人为研究对象的文献,所以一方面需要扩大25-(OH)D水平与结直肠癌在不同种族人群中的研究,另一方面,有研究表明1,25-二羟基维生素D3能增强卡铂对人肺癌A549细胞的杀伤效果[25],因此应深入研究25-(OH)D在结直肠癌进展中的作用机制,为结直肠癌的防治提供借鉴。
| [1] | Chen Q, Liu ZC, Chen LP, et al. An analysis of incidence and mortality of colorectal cancer in china, 2003-2007[J]. Zhongguo Zhong Liu, 2012, 21(3):179-82. [陈琼, 刘志才, 程兰平, 等. 2003-2007年中国结直肠癌发病与死亡分析[J]. 中国肿瘤, 2012, 21(3): 179-82.] |
| [2] | Garland CF, Garland FC. Do sunlight and vitamin D reduce the likelihood of colon cancer?[J]. Int J Epidemiol, 1980, 9(3): 227-31. |
| [3] | Evans SR, Shchepotin EI, Young H, et al. 1,25-dihydroxyvitamin D3 synthetic analogs inhibit spontaneous metastases in a 1,2-dimethylhydrazine-induced colon carcinogenesis model[J]. Int J Oncol, 2000, 16(6):1249-54. |
| [4] | Newmark HL, Yang K, Kurihara N, et al. Western-style dietinduced colonic tumors and their modulation by calcium and vitamin D in C57Bl/6 mice: a preclinical model for human sporadic colon cancer[J]. Carcinogenesis, 2009, 30(1): 88-92. |
| [5] | Diaz GD, Paraskeva C, Thomas MG, et al. Apoptosis is induced by the active metabolite of vitamin D3 and its analogue EB1089 in colorectal adenoma and carcinoma cells: possible implications for prevention and therapy[J]. Cancer Res, 2000, 60(8): 2304-12. |
| [6] | Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement[J]. Int J Surg, 2010, 8(5): 336-41. |
| [7] | GA Wells, B Shea, D O’Connell, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in metaanalyses[S]. http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed 30 April 2013. |
| [8] | Higgins JP, Thompson SG. Quantifying heterogeneity in a metaanalysis[J]. Stat Med, 2002, 21(11): 1539-58. |
| [9] | Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses[J]. BMJ, 2003, 327(7414): 557-60. |
| [10] | Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test[J]. BMJ, 1997, 315(7109): 629-34. |
| [11] | Neuhouser ML, Manson JE, Millen A, et al. The influence of health and lifestyle characteristics on the relation of serum 25-hydroxyvitamin D with risk of colorectal and breast cancer in postmenopausal women[J]. Am J Epidemiol, 2012, 175(7): 673-84. |
| [12] | Lee JE, Li H, Chan AT, et al. Circulating levels of vitamin D and colon and rectal cancer: the Physicians’ Health Study and a metaanalysis of prospective studies[J]. Cancer Prev Res (Phila), 2011, 4(5): 735-43. |
| [13] | Jenab M, Bueno-de-Mesquita HB, Ferrari P, et al. Association between pre-diagnostic circulating vitamin D concentration and risk of colorectal cancer in European populations: a nested casecontrol study[J]. BMJ, 2010, 340: b5500. |
| [14] | Wu K, Feskanich D, Fuchs CS, et al. A nested case-control study of plasma 25-hydroxyvitamin D concentrations and risk of colorectal cancer[J]. J Natl Cancer Inst, 2007, 99(14): 1120-9. |
| [15] | Feskanich D, Ma J, Fuchs CS, et al. Plasma vitamin D metabolites and risk of colorectal cancer in women[J]. Cancer Epidemiol Biomarkers Prev, 2004, 13(9): 1502-8. |
| [16] | Otani T, Iwasaki M, Sasazuki S, et al. Plasma vitamin D and risk of colorectal cancer: the Japan Public Health Center-Based Prospective Study[J]. Br J Cancer, 2007, 97(3): 446-51. |
| [17] | Weinstein SJ, Yu K, Horst RL, et al. Serum 25-hydroxyvitamin D and risks of colon and rectal cancer in Finnish men[J]. Am J Epidemiol, 2011, 173(5): 499-508. |
| [18] | Woolcott CG, Wilkens LR, Nomur a AM, et al. Plasma 25-hydroxyvitamin D levels and the risk of colorectal cancer: The multiethnic cohort study[J]. Cancer Epidemiol Biomarkers Prev, 2010, 19(1): 130-4. |
| [19] | Trivedi DP, Doll R, Khaw KT. Effect of four monthly oral vitamin D3 (cholecalciferol) supplementation on fractures and mortality in men and women living in the community: randomized double blind controlled trial[J]. BMJ, 2003, 326(7387): 469. |
| [20] | Giovannucci E. Epidemiology of vitamin D and colorectal cancer [J]. Anticancer Agents Med Chem, 2013, 13(1): 11-9. |
| [21] | Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an endocrine society clinical practice guideline[J]. J Clin Endocrinol Metab, 2011, 96(7): 1911-30. |
| [22] | Slattery ML, Neuhausen SL, Hoffman M, et al. Dietary calcium, vitamin D, VDR genotypes and colorectal cancer[J]. Int J Cancer, 2004, 111(5): 750-6. |
| [23] | Slattery ML, Wolff RK, Herrick JS, et al. Calcium, vitamin D, VDR genotypes,and epigenetic and genetic changes in rectal tumors[J]. Nutr Cancer, 2010, 62(4): 436-42. |
| [24] | Huncharek M, Muscat J, Kupelnick B. Colorectal cancer risk and dietary intake of calcium, vitamin D, and dairy products: a metaanalysis of 26,335 cases from 60 observational studies[J]. Nutr Cancer, 2009, 61(1): 47-69. |
| [25] | Hu ZY, Zhou YP, Li SW, et al. 1,25-digydroxyvitaminD3 enhanced killing effect of carboplatin on growth in lung cancer cell A549[J]. Zhong Liu Fang Zhi Yan Jiu, 2013, 40(2): 125-30. [胡志勇, 周逸鹏, 黎书炜, 等. 1,25-二羟基维生素D3增强卡铂对人肺癌A549细胞的杀伤效果[J]. 肿瘤防治研究, Zhong Liu Fang Zhi Yan Jiu, 2013, 40(2): 125-30.] |