 2014, Vol.41
2014, Vol.41

2. 广西医科大学附属肿瘤医院肿瘤外 科;
3. 广西医科大学第十附属医院肿瘤内科


2.Department of Surgical Oncology,The Tumor Hospital of Guangxi Medical University;
3.Department of Medical Oncology,The Tenth Affiliated Hospital of Guangxi Medical University
Corresponding Author:ZHONG Jianhong,E-mail:zhongjianhong66@163.com (* :Contributed Equally As First Author)
乳腺癌(breast cancer,BC)侵袭性强,已成 为威胁女性生命健康的第二大肿瘤[1]。其发病率 呈逐年上升的趋势,全世界每年有超过100万的 新发病例[2],而发达国家的发病率明显高于发展 中国家[3]。然而,BC的发病机制尚未完全清楚, 目前多认为由多环境与多基因共同作用所致[4]。 其中,基因多态性是BC发病的一个非常重要的流 行病因素。最近,两个较大的研究[5, 6]发现很多潜在的基因多态性与BC密切相关,其中包括了8q24 rs13281615基因多态性。
自2007年报道了8q24 rs13281615 基因多态性 和肿瘤的发病关系之后,有很多流行病学研究评 价rs13281615基因多态性和BC的发病关系。但 结果不尽相同,有必要采取Meta分析的方法探讨 rs13281615基因多态性与BC易感性的关系。 1 资料与方法 1.1 文献检索
中文以乳腺癌、rs13281615、多态性,英文以 BC/breast neoplasm/breast cancer,8q24/rs13281615/ SNP/single nucleotide polymorphism为主题词、关 键词,分别在中国学术期刊全文数据库、维普中 文科技期刊数据库、万方全文数据库及PubMed 和EMBASE数据库上进行检索,检索日期截止到 2012年12月,收集研究rs13281615基因多态性与 BC易感性的病例对照研究。 1.2 文献纳入标准
(1)国内外关于rs13281615基因多态性与BC 易感性的病例-对照研究;(2)研究方法相同或相 似,能提供病例组和对照组的人数、基因型的频 率分布及相关的原始数据;(3)BC病例均经组织 病理学确诊。 1.3 统计学方法
两个评价员按Meta分析的要求分别收集、整 理、核实及校对数据。采用RevMan 5.14统计软件 进行Meta分析,对文献结果进行异质性检验(Q 检验),若P>0.10表示结果一致性较好,采用固 定效应模型进行数据分析;反之,P<0.10则采用 随机效应模型进行效应量的合并。以风险比(risk ratio,OR) 及其95%CI作为每个研究结果的研究效 应测定指标。Hardy-Weinberg Equilibrium (HWE) 采用http://krunch.med.yale.edu/hwsim/网站提供的 免费程序HWSIM来进行计算,以α=0.05为检验水 准,P>0.05时表示群体基因遗传平衡,数据来自同 一蒙德尔群体,且具有代表性;P<0.05表示群体缺 乏代表性。采用敏感度分析评价结果的稳定性,对 纳入的文献使用倒漏斗图进行发表偏倚评价。 2 结果 2.1 文献概述
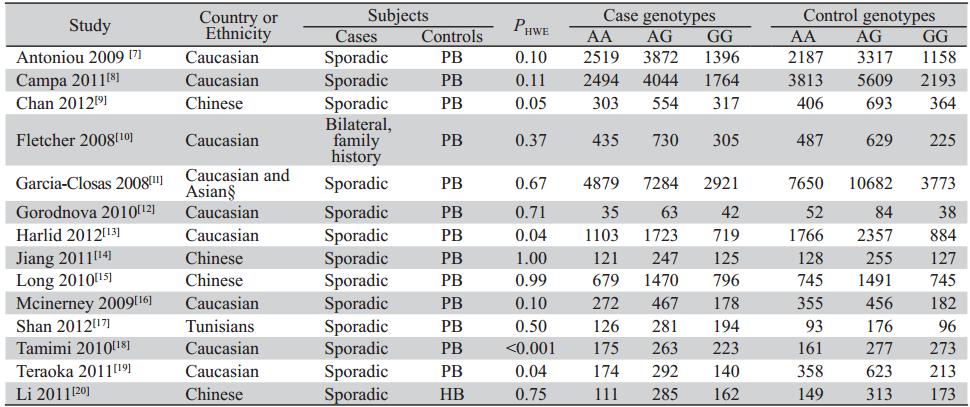
共检索符合纳入标准的文献14篇[7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20],其中4 篇为中国人群,10篇为高加索人和黑人,包括13 篇英文文献及1篇中文文献,累计病例44 283例, 对照55756例。纳入研究的基本特点见表1。
|
|
表1 纳入文献中观察组与对照组的一般资料 Table 1Characteristic of selected studies about the association between 8q24 rs13281615 SNP and the susceptibility of breast cancer included in this study |
GG基因型与AG+AA基因型比较,GG基因型 与AA基因型比较,G等位基因与A等位基因比较 和AA基因型与GA+GG基因型比较的发表偏倚均 采用RevMan5.14软件进行分析。漏斗图显示研究 间分布不均匀,可能存在发表偏倚。 2.3 Meta分析结果 2.3.1 G等位基因与A等位基因比较
计算罹患BC 的OR值及95%CI。异质性检验P<0.001,I2=67%, 存在异质性,采用随机效应模型计算,OR=1.10,95%CI=1.06~1.14,P<0.001,见图1,说明G等位基 因型罹患BC是A等位基因型的1.10倍。
 | 图1 rs13281615基因多态性与BC易感性关系的Meta分析森林图(G等位vs. A等位)Figure 1 Forest plots describing the association of rs13281615 gene polymorphism with breast cancer (G-allele vs. A-allele) |
计算罹患BC的 OR值及95%CI。异质性检验P=0.006,I2=56%,存 在异质性,故采用随机效应模型计算,OR=1.20, 95%CI=1.16~1.24,P<0.001,说明GG基因型罹患 BC是AA基因型的1.20倍。 2.3.3 以AG+AA基因型为参照计算GG基因型个 体罹患BC的OR值及95%CI
异质性检验P=0.05、 I2=42%,故采用随机效应模型合并分析。合并OR 值为1.13 ( 95%CI=1.08~1.19,P<0.001),说明GG基 因型个体罹患BC的风险是AG+AA基因型个体的 1.13倍。 2.3.4 AA与AG+GG比较
计算罹患BC的OR值 及95%CI。异质性检验P=0.01,I2=51%,存在 异质性,采用随机效应模型计算,OR=0.89, 95%CI=0.84~0.93,P<0.001,说明AA基因型罹患 BC是AG+GG基因型的0.89倍。 2.4 亚组分析 2.4.1 混合人群
GG vs.AG+AA;GG vs.AA; AA vs.AG+GG;G等位 vs.A等位基因型,异质性检 验显示P均<0.1,故采用随机效应模型。合并OR 值分别为1.15 (95%CI:1.07~1.22,P<0.001);1.22 (95%CI:1.12~1.33,P<0.001);0.88(95%CI:0.83~0.94, P<0.001);1.11(95%CI:1.06~1.17,P<0.001)。 2.4.2 中国人群
GG vs.AG+AA; GG vs.AA; AA vs.AG+GG;G等位vs.A等位基因型,异质性 检验均显示P>0.05,I2=0,各研究间同质性好,采 用固定效应模型。合并OR值分别为1.10(95%CI: 1.01~1.20,P=0.03);1.17(95%CI=1.05~1.30, P=0.005);0.90(95%CI:0.82~0.98,P=0.02);1.07 (95%CI:1.02~1.13,P=0.01)。 2.5 敏感度分析
使用固定效应模型和随机效应模型对研究结 果进行比较,探讨结果的稳定性,发现结果可 靠,见表2。
|
|
表2 Meta分析结果敏感度分析 Table 2 Sensitivity analysis for total population |

BC是环境与宿主相互作用、多基因参与的复 杂性疾病。目前流行病学认为内分泌因素、家族 遗传与其发病率相关,很多BC散发于人群中。因 此,基因多态性可能参与了BC的发生及发展, Meta分析也证实了基因多态性与BC存在很大的关 联性[21, 22]。
目前普遍认为的BRCA1及BRCA2基因多态 性与BC相关,但是由于其较低的突变率[23],因 此只能在小部分的BC患者中检出。2007年,全 基因组关联分析鉴定出很多基因多态性可能与 BC的发生发展相关,包括了rs13281615。但是后 期对于rs13281615与BC的研究结果缺乏一致性, 宋俊颖等[24]纳入7个研究病例约50 000例,Meta 分析结果显示G等位基因可能会增加BC罹患风险 (OR=1.14,95%CI:1.04~1.25,P=0.007),其亚组 分析结果认为这种罹患风险在欧洲妇女尤其明显 (OR=1.14,95%CI:1.02~1.28,P=0.02),而亚洲妇 女的风险却不明显(OR=1.13,95%CI:0.93~1.38, P=0.23)。随后报道的几个样本量更大的病例-对 照研究亦评估了该基因与BC的关系,但结论却很 不一致。为此,我们进行了更为系统的检索,共 纳入14个研究,总样本量高达100000例,为之前 研究的两倍,使结果更具有说服力。本研究结果 显示:GG基因型显著增加罹患BC的风险性,而 AA基因型则降低其风险,对中国人群以及混合人 群(95%以上为高加索人群)进行亚组分析,结果 亦然,P值显示均具有统计学意义。敏感度分析结 果一致。
纳入的很多研究在设计上都考虑了宿主的多 重因素的相互作用,只有1篇研究[7]评估rs13281615 基因多态性与BC关系的时候考虑到了BRCA1及 BRCA2多态性的相互作用。所纳入的这些研究都 证明了BC的发病机制包含了宿主与环境因素的相 互协同作用。
BC是一种在不同人种中其发病率及死亡率具 有差异的多混杂因素的疾病[25]。每增加25%欧洲血 统,其罹患BC的风险将增加1.79倍[26]。有研究显 示,在北美及欧洲国家BC的发病率是亚洲国家的3 倍[27];Easton等[6]认为欧洲人群发病率高于其他种 族人群;本研究结果与这些研究的观点一致。欧 洲及北美国家具有较高的BC发病率。而本研究结 果显示混合人群罹患BC的风险比中国人群更高。 然而,G等位基因频率在中国人群中的分布却高 于混合人群。这种不一致可能与BC是混杂多因素 参与的疾病有关。因此,任何一个单独的基因多 态性(包括rs13281615)都不能单独引起BC的发 生,仅是增加其发病风险。
本文存在一定的局限性。首先,尽管对照组 均为健康人群,但是均不能明确进行定义,且部 分研究不符合HWE定律,其人群缺乏代表性。其 次,BC是多因素致病,而本文纳入的研究由于 缺乏需要的原始数据而不能通过在年龄、激素水 平、绝经年龄等方面进行分层亚组分析。最后, 由于缺乏原始数据,因此无法对这些研究进行基 因-环境、基因-基因的潜在相互作用进行分析。 即便如此,本研究显示GG基因型可以增加 个体罹患BC的风险,AA基因型是BC的保护型基 因。但是由于存在以上的局限性,以后尚需从基 因-基因及基因-环境方面进行更大样本、更严谨的 研究,从而得到更可靠的证据,为BC提供更进一 步的防治措施及治疗方案。
| [1] | Smigal C, Jemal A, Ward E, et al. Trends in breast cancer by race and ethnicity: update 2006[J]. CA Cancer J Clin, 2006, 56(3): 168-83. |
| [2] | Jemal A, Bray F, Center MM, et al.Global cancer statistics[J].CA Cancer J Clin,2011,61(2):69-90. |
| [3] | Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics, 2002[J]. CA Cancer J Clin, 2005, 55(2): 74-108. |
| [4] | Lichtenstein P, Holm NV, Verkasalo PK, et al. Environmental and heritable factors in the causation of cancer--analyses of cohorts of twins from Sweden, Denmark, and Finland[J]. N Engl J Med, 2000, 343(2): 78-85. |
| [5] | Hunter DJ, Kraft P, Jacobs KB, et al. A genome-wide association study identifies alleles in FGFR2 associated with risk of sporadic postmenopausal breast cancer[J]. Nat Genet, 2007, 39(7): 870-4. |
| [6] | Easton DF, Pooley KA, Dunning AM, et al. Genome-wide association study identifies novel breast cancer susceptibility loci[J]. Nature, 2007, 447(7148): 1087-93. |
| [7] | Antoniou AC, Sinilnikova OM, McGuffog L, et al. Common variants in LSP1, 2q35 and 8q24 and breast cancer risk for BRCA1 and BRCA2 mutation carriers[J]. Hum Mol Genet, 2009, 18(22): 4442-56. |
| [8] | Campa D, Kaaks R, Le Marchand L, et al. Interactions between genetic variants and breast cancer risk factors in the breast and prostate cancer cohort consortium[J]. J Natl Cancer Inst, 2011, 103(16): 1252-63. |
| [9] | Chan M, Ji SM, Liaw CS, et al. Association of common genetic variants with breast cancer risk and clinicopathological characteristics in a Chinese population[J]. Breast Cancer Res Treat, 2012, 136(1): 209-20. |
| [10] | Fletcher O, Johnson N, Gibson L, et al. Association of genetic variants at 8q24 with breast cancer risk[J]. Cancer Epidemiol Biomarkers Prev, 2008, 17(3): 702-5. |
| [11] | Garcia-Closas M, Hall P, Nevanlinna H, et al. Heterogeneity of breast cancer associations with five susceptibility loci by clinical and pathological characteristics[J]. PLoS Genet, 2008, 4(4): e1000054. |
| [12] | Gorodnova TV, Kuligina E, Yanus GA, et al. Distribution of FGFR2, TNRC9, MAP3K1, LSP1 and 8q24 alleles in genetically enriched breast cancer patients versus elderly tumor-free women[J]. Cancer Genet Cytogenet, 2010, 199(1): 69-72. |
| [13] | Harlid S, Ivarsson MI, Butt S, et al. Combined effect of lowpenetrant SNPs on breast cancer risk[J]. Br J Cancer, 2012, 106(2): 389-96. |
| [14] | Jiang Y, Han J, Liu J, et al. Risk of genome-wide association study newly identified genetic variants for breast cancer in Chinese women of Heilongjiang Province[J]. Breast Cancer Res Treat, 2011, 128(1): 251-7. |
| [15] | Long J, Shu XO, Cai Q, et al. Evaluation of breast cancer susceptibility loci in Chinese women[J]. Cancer Epidemiol Biomarkers Prev, 2010, 19(9): 2357-65. |
| [16] | McInerney N, Colleran G, Rowan A, et al. Low penetrance breast cancer predisposition SNPs are site specific[J]. Breast Cancer Res Treat, 2009, 117(1): 151-9. |
| [17] | Shan J, Mahfoudh W, Dsouza SP, et al. Genome-Wide Association Studies (GWAS) breast cancer susceptibility loci in Arabs: susceptibility and prognostic implications in Tunisians[J]. Breast Cancer Res Treat, 2012, 135(3): 715-24. |
| [18] | Tamimi RM, Lagiou P, Czene K, et al. Birth weight, breast cancer susceptibility loci, and breast cancer risk[J]. Cancer Causes Control, 2010, 21(5): 689-96. |
| [19] | Teraoka SN, Bernstein JL, Reiner AS, et al. Single nucleotide polymorphisms associated with risk for contralateral breast cancer in the Women's Environment, Cancer, and Radiation Epidemiology (WECARE) Study[J]. Breast Cancer Res, 2011, 13(6): R114. |
| [20] | Li LH, Guo ZJ, Hua D, et al. Association of the 8q24 rs13281615 polymorphisms with breast cancer risk and Clinical and Pathological Characteristics in Chinese Han Women[J]. Zhonghua Jian Yan Yi Xue Za Zhi,2011,34(1): 73-6. [李莉华, 郭子健, 华东等. 8q24 rs13281615基因多态性与中国汉族女性乳腺癌患病风险及临床病理特征的关系[J]. 中华检验医学杂志, 2011, 34(1): 73-6. ] |
| [21] | Saadat M. Paraoxonase 1 genetic polymorphisms and susceptibility to breast cancer: A meta-analysis[J]. Cancer Epidemiol, 2012, 36(2): e101-3. |
| [22] | Pabalan N, Jarjanazi H, Sung L,et al. Menopausal Status Modifies Breast Cancer Risk Associated with the Myeloperoxidase (MPO) G463A Polymorphism in Caucasian Women: A Meta-Analysis[J]. PLoS One, 2012, 7(3):e32389. |
| [23] | Walsh T, Casadei S, Coats KH, et al. Spectrum of mutations in BRCA1, BRCA2, CHEK2, and TP53 in families at high risk of breast cancer[J]. JAMA, 2006, 295(12): 1379-88. |
| [24] | Song JY,Zhang LN,Zheng H,et al. Association between a single nucleotide polymorphism in 8q24 rs13281615 and breast cancer risk: a Meta-analysis[J].Zhong Liu,2012,32(1):38-41,64.[宋俊颖, 张丽娜, 郑红, 等. 8q24 rs13281615单核苷酸多态性与乳腺癌发病风险的Meta分析[J]. 肿瘤, 2012, 32(1): 38-41,64.] |
| [25] | McCracken M, Olsen M, Chen MS Jr, et al. Cancer incidence, mortality, and associated risk factors among Asian Americans of Chinese, Filipino, Vietnamese, Korean, and Japanese ethnicities[J]. CA Cancer J Clin, 2007, 57(4): 190-205. |
| [26] | Ziv E, John EM, Choudhry S, et al. Genetic ancestry and risk factors for breast cancer among Latinas in the San Francisco Bay Area[J]. Cancer Epidemiol Biomarkers Prev, 2006, 15(10): 1878-85. |
| [27] | Jemal A, Bray F, Center MM, et al. Global cancer statistics[J]. CA Cancer J Clin, 2011, 61(2): 69-90 |