 2014, Vol.41
2014, Vol.41



20世纪80年代Hodge等提出的系统前列腺6点 法活组织检查以及后来的经直肠超声(transrectal ultrasound,TRUS)引导穿刺术都对前列腺癌诊断 具有里程碑意义。随着研究的不断深入,对于前列 腺穿刺的理念不断被更新,12点法、饱和24点法系 统活检[1]被越来越多的医生所采纳。但是,穿刺针 数的增加带来了并发症风险的相继增加[2],不仅对 患者的创伤加大,而且增加了医务工作者的负担。 本文通过回顾性研究复旦大学附属中山医院泌尿 外科TRUS引导下经会阴前列腺穿刺的病例,比较 不同血清前列腺特异抗原(prostate specifi c antigen, PSA)水平的患者采用6点法和12点法首次前列腺 穿刺活检阳性率,探讨针对不同的患者人群设计国 人合理的穿刺点数,现报告如下。 1 资料与方法 1.1 研究对象
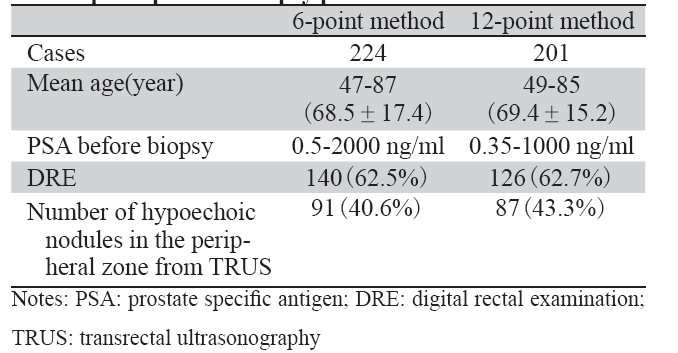
本组纳入了2011年10月至2012年1月间6点法 穿刺的患者224例以及2012年4月至2012年7月间 12点法穿刺的患者201例,共425例,均为首次前 列腺穿刺活检的患者,其中排除了穿刺前服用保 列治或抗雄激素治疗的患者。两组患者的年龄、 穿刺前PSA等临床资料,见表1。所有患者均符合 《中国泌尿外科疾病诊断治疗指南》[3]描述的前列 腺穿刺活检指征。
|
|
表1 前列腺6点和12点法穿刺患者临床资料的比较 Table 1 Comparison of clinical characteristics of 6-point and 12-point prostate biopsy patients |
6点法是指在前列腺左右叶的上、中、下部 各穿刺1点。12点法采用前列腺左右叶旁矢状面 (内、外侧)各2针及前外侧角、移行带各1针, 图中蓝色穿刺点在矢状面上取前后2针,见图1。 所有穿刺均采用TRUS引导下经会阴穿刺的方法。 术前口服抗菌药3天。进针位点位于肛门上缘以上 2 cm正中线旁开1.5 cm处。先从该位点进针注射 1%利多卡因至前列腺包膜下行局部麻醉,然后采 用Bard活组织检查枪取出前列腺左右叶组织。穿 刺后局部压迫止血并继续服用抗菌药3天。
 |
图1 前列腺不同穿刺方法示意图 Figure 1 Schematic of different methods of prostate biopsy |
超声诊断仪为丹麦产,型号BK2102,直肠探头为10M平面及8M扇形扫描双切面探头。 1.4 统计学方法
应用stata 10.0统计学软件。对各组数据以 Pearson卡方检验或Fisher确切概率法进行统计学检 验。P<0.05为差异具有统计学意义。 2 结果 2.1 病理检查结果
425例患者中,前列腺穿刺活检的病理结果显 示前列腺癌234例(53.8%),前列腺肉瘤1例, 其余190例均为良性病变,如低级别前列腺上皮 内瘤(prostatic intraepithelial neoplasia,PIN)、 前列腺小腺泡不典型增生(atypical small acinar proliferation of prostate,ASAP)、良性前列腺增 生、急慢性前列腺炎等。 2.2 不同PSA水平的活检阳性率情况
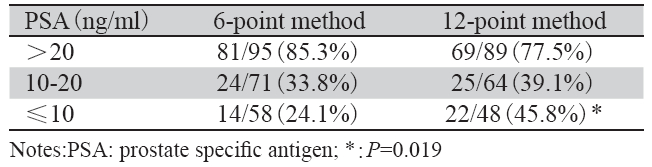
患者按术前PSA水平分组,首次活检阳性率 PSA>20 ng/ml组6点法高于12点法,差异无统计 学意义(P=0.177);PSA10~20 ng/ml组12点法高 于6点法,差异无统计学意义(P=0.526);PSA≤ 10 ng/ml组12点法高于6点法,差异有统计学意义 (P=0.019),见表2。因此,若PSA>20 ng/ml, 可采用6点法穿刺活检;PSA≤10 ng/ml可采用12点 法穿刺活检,而PSA10~20 ng/ml则两种穿刺方法 均可采用。
|
|
表2 不同PSA水平6点和12点穿刺法患者首次活检阳性率比较 Table 2 Comparison of positive rate of 6- and 12-point methods of fi rst prostate biopsy at different PSA levels |
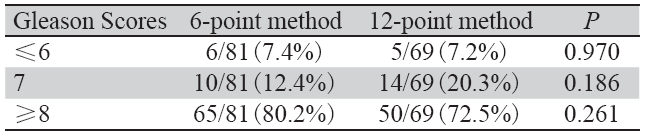
PSA>20 ng/ml组中,6点法与12点法Gleason 评分的情况比较,差异无统计学意义,见表3。结 果表明穿刺点与Gleason评分无关,但从减少患者 伤害的角度,PSA>20 ng/ml的患者6点法比12点法 更适宜。
|
|
表3 PSA>20 ng/ml患者的Gleason评分情况 Table 3 Gleason score of patients with PSA>20 ng/ml |
PSA>20 ng/ml组前列腺癌根治术22例,其中 新辅助后根治术7例,其余15例术后标本病理显 示PT2c1例(6.7%),PT3a6例(40%),PT3b4 例(26.7%),阳性切缘4例(26.7%)。结果显示, PSA>20 ng/ml患者根治术后标本病理T3明显高于 T2,且有切缘阳性。 2.5 PSA≤20 ng/ml患者穿刺活检Gleason评分与前 列腺癌根治术后病理Gleason评分比较
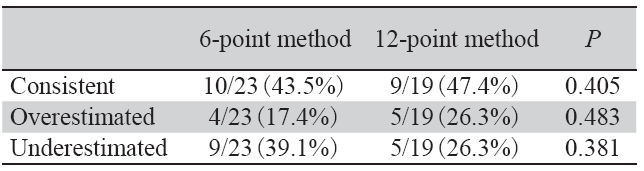
PSA≤20 ng/ml患者前列腺癌根治术共42例, 其中术前6点法23例,12点法19例。结果显示,12 点法活检Gleason 评分与术后病理Gleason 评分一 致性更高,但差异无统计学意义;12点法降低了 穿刺活检Gleason评分低估率,但差异无统计学意 义,见表4。
|
|
表4 PSA≤20 ng/ml前列腺患者活检与术后病理Gleason评分比较 Table4 Comparison of Gleason score before and after surgery of PSA≤20 ng/ml patients |
两种不同穿刺方法均未出现患者感染性休
克、脓毒血症、大出血等严重并发症。术后尿潴
留和严重出血需膀胱连续冲洗的患者少见,6点法
与12点法尿潴留的发生率分别为0.45%(1例)和
0.50%(1例),严重出血发生率分别为0.89%(2
例)和1.00%(2例)。
3 讨论/span>
前列腺穿刺活检已成为公认的诊断前列腺癌
的“金标准”[4]。而经直肠超声(TRUS)可获得前
列腺横断面和矢状面的清晰图像,实时监测整个
穿刺过程。因此,自上世纪80年代以来,TRUS
引导下的前列腺穿刺活检术得到了广泛应用。然
而,TRUS引导下的前列腺穿刺结果受到前列腺穿
刺针数的影响。就穿刺针数而言,目前还没有形
成统一的意见。一般认为初次穿刺时多于12点的
穿刺不但未提高前列腺癌的检出率,而且多于18
点的穿刺可能会引起严重并发症[2]。根据年龄、前
列腺体积、直肠指检(DRE),推荐不同的穿刺针
数[5]。血清PSA对前列腺癌有重要的诊断意义,PSA
水平与前列腺癌穿刺阳性率有很强的相关性[6]。但
是,目前大多数相关研究以欧美人群为主,Yoon
等[7]提出欧美人群的PSA预测穿刺阳性的标准并不
适用于亚洲人。所以,探究适用于我国人群的穿
刺针数标准是很有价值的。
本研究中观察到对于PSA>20 ng/ml的患者,
6点法和12点法穿刺活检阳性率都很高,分别为
85.3%和77.5%,两者比较差异没有统计学意义。
结果可能与两个因素有关,第一,PSA>20 ng/ml
的人群患前列腺癌的风险较PSA≤20 ng/ml的人群
高,所以穿刺的阳性率会较高;第二,PSA与肿
瘤的分级分期有关,PSA高的患者通常都有较高
的Gleason评分和较高的临床分期,这使得前列腺
穿刺可能更容易发现肿瘤。本研究的结果也证实
了以上看法。此外,从前列腺癌根治术后病理来
看,PSA>20 ng/ml的患者中,除7例新辅助治疗
的病例外,其余15例临床分期为T2c或T3,也就
是说肿瘤浸润或突破包膜,这为穿刺到肿瘤提供
了有利条件,6针穿刺即能容易地发现肿瘤,而12
针穿刺法多加的6针并未提高检出的阳性率。从指
导临床治疗的角度来看,本研究中PSA>20ng/ml
的穿刺结果阳性患者中,无论6点法还是12点法,
两者的Gleason评分差异无统计学意义,说明穿刺
点数与Gleason评分无关,6点法与12点法在诊断
PSA>20 ng/ml的患者时是等价的,但从减少对患
者伤害的角度出发,6点法较12点法更适宜。吴嘉
等[8]研究也支持上述观点,在回顾300例患者后认
为对PSA>20 ng/ml的人群可采用6点穿刺法,或
可再对可疑部位追加1~2针。
本研究还发现在PSA≤10 ng/ml患者中12点
法较6点法阳性率明显增加(P=0.019)。近年
来,对于PSA10~20 ng/ml与PSA≤10 ng/ml患者寻
找最佳穿刺针数的研究颇多。Eichler等[2]研究发
现,初次穿刺时多于12点的穿刺不但未提高前列
腺癌的检出率,而且多于18点的穿刺可能会引起
严重并发症。Scattoni等[5]对617例患者进行24点
前列腺系统穿刺,发现10~16针穿刺方案可获得
最佳穿刺结果。Delongchamps等[9]的研究显示,
超过18点的饱和穿刺法并不能提高前列腺癌的检
出率。而Novara等[10]对143例既往活检阴性的患
者进行了24针前列腺饱和穿刺活检,筛检阳性率
为28%。Zaytoun等[11]采用24针经直肠径路前列腺
饱和穿刺活检对既往阴性活检的患者进行筛检,
其前列腺癌筛检阳性率达32.7%,优于14针方案
(29.7%)。饱和24针系统活检都集中于首次阴性活检的病例。从成本和效率来看,饱和24针系统
穿刺需要静脉或椎管麻醉,需穿刺模板引导,大
大延长了手术时间、增加了患者的手术风险,目
前尚难在首次穿刺中广泛开展。另有文献报道随
着前列腺穿刺活检位点数目的增加,不仅前列腺
癌的筛检阳性率相应增加,而且穿刺结果Gleason
评分与术后病理Gleason 评分更加一致[12, 13]。本研
究观察到12点法与6点法相比,12点法穿刺Gleason
评分与术后病理Gleason 评分一致性更高,但是差
异无统计学意义,这个观点有待未来更大样本量
的研究。
综上所述,对于首次行前列腺穿刺活检的国
人,若PSA>20 ng/ml推荐行6点法穿刺,而PSA≤
10 ng/ml推荐12点法穿刺。至于PSA10~20 ng/ml两
种穿刺方法均可选用,而更大样本量的研究有助
于进一步比较穿刺活检阳性率以及穿刺Gleason 评
分与术后病理Gleason 评分的一致性。
| [1] | Zhang FB, Shao Q, Du Y, et al. Ultrasound-guided transperinea1 24-core saturation prostate biopsy is superior to the 14-core scheme in detecting prostate cancer in patients with PSA<20 μg/ L[J]. Zhonghua Nan Ke Xue Za Zhi,2012,18(4):306-9. [张峰波, 邵强,杜源,等. 经会阴前列腺24针饱和穿刺活检与14针活检 在PSA<20 μg/L患者中筛检前列腺癌的对比性研究[J]. 中华男 科学杂志,2012,18(4):306-9.] |
| [2] | Eichler K, Hempel S, Wilby J, et al. Diagnostic value of systematic biopsy methods in the investigation of prostate cancer: a systematic review[J]. J Urol,2006,175(5):1605-12. |
| [3] | Na YQ, Ye ZQ, Sun G, et al. Guideline to diagnosis and treatment of urological diseases China[M]. Beijing: People's Health Publishing House, 2011:51. [那彦群,叶章群,孙光,等. 中国 泌尿外科疾病诊断治疗指南手册[M]. 北京:人民卫生出版 社,2011:51.] |
| [4] | Hodge KK, McNeal JE, Stamey TA. Ultrasound guided transrectal core biopsies of the palpably abnormal prostate[J]. J Urol,1989,142(1):66-70. |
| [5] | Scattoni V, Raber M, Abdollah F, et al. Biopsy schemes with the fewest cores for detecting 95% of the prostate cancers detected by a 24-core biopsy[J]. Eur Urol,2010,57(1):1-8. |
| [6] | Thompson IM, Ankerst DP, Chi C, et al. Operating characteristics of prostate-specifi c antigen in men with an initial PSA level of 3.0 ng/ml or lower[J]. JAMA,2005,294(1):66-70. |
| [7] | Yoon DK, Park JY, Yoon S, et al. Can the prostate risk calculator based on Western population be applied to Asian population?[J]. Prostate,2012,72(7):721-9. |
| [8] | Wu J, Ma YZ, Chen Z, et al. Comparison of 6 o'clock and 12 o'clock position prostate biopsy cores for detection of prostate cancer:a retrospective analysis[J]. Shanghai Yi Xue,2011,34(7):532-5.[ 吴 嘉,马扬之,陈忠,等. 6点与12点前列腺穿刺活组织检查诊断前 列腺癌的回顾性比较分析[J]. 上海医学,2011,34(7):532-5.] |
| [9] | Delongchamps NB, de la Roza G, Jones R, et al. Saturation biopsies on autopsied prostates for detecting and characterizing prostate cancer[J]. BJU Int,2009,103(1):49-54. |
| [10] | Novara G, Boscolo-Berto R, Lamon C, et al. Detection rate and factors predictive the presence of prostate cancer in patients undergoing ultrasonography-guided transperineal saturation biopsies of the prostate[J]. BJU Int,2010,105(9):1242-6. |
| [11] | Zaytoun OM, Moussa AS, Gao T, et al. Offi ce based transrectal saturation biopsy improves prostate cancer detection compared to extended biopsy in the repeat biopsy population[J]. J Urol,2011,186(3):850-4. |
| [12] | Emiliozzi P, Maymone S, Paterno A, et al. Increased accuracy of biopsy Gleason score obtained by extended needle biopsy[J]. J Urol,2004,172(6 Pt 1):2224-6. |
| [13] | King CR, McNeal JE, Gill H, et al. Extended prostate biopsy scheme improves reliability of Gleason grading: implications for radiotherapy patients[J]. Int J Radiat Oncol Biol Phys,2004,59(2):386-91. |