 2014, Vol.41
2014, Vol.41



近年来我国新发现的前列腺癌患者数量逐年 增加,得益于前列腺特异性抗原(prostate specific antigen,PSA)筛查的普及,越来越多的早期前列腺 癌患者被发现,但是仍有许多患者发现时就属于 晚期[1, 2, 3],失去了根治性手术的机会。据统计,我 国13.3%~26%新发现的前列腺癌患者在确诊时即 有骨转移,高于西方国家[4, 5]。全世界因前列腺癌 死亡的患者中有85%发生了骨转移。大约50%的前 列腺癌骨转移患者在确诊后30~35月内死亡[6, 7, 8]。99mTc亚甲基二膦酸盐(technetium 99mTc methylene diphosphonate,99mTc-MDP)骨显像是最常用的检 测骨转移方法。放射性核素全身骨显像检查(ECT bone scan)对探查前列腺癌骨转移是一种较灵敏的 方法,研究证实,骨显像较X线提前3到6月发现病 变[9]。由于前列腺的骨转移绝大多数为成骨性转 移,全身骨显像对早期骨转移有很高的诊断价值。 2011版中国泌尿外科指南指出一旦前列腺癌诊断 成立,建议进行全身核素骨显像检查,特别是在 PSA>20 ng/ml,Gleason评分大于7分的病例[10]。由 于前列腺癌转移的病变骨骼的血流、代谢和功能 的早期改变,放射性核素骨显像在寻找骨转移灶 方面有非常高的敏感度,但是骨显像检查假阳性 率很高,特异性较差。另外,全身骨显像检查成 本高、检查时间长,而且具有放射性。因此,前 列腺癌患者骨转移的早期发现需要具有更高特异 性、更便于随访的筛查手段来协助。
近年来国内外学者研究发现,对于前列腺癌 患者,某些血清学标志物的浓度变化与骨转移有 密切的相关性。本文综述与前列腺癌骨转移相关 的血清学证据。 1 前列腺特异性抗原
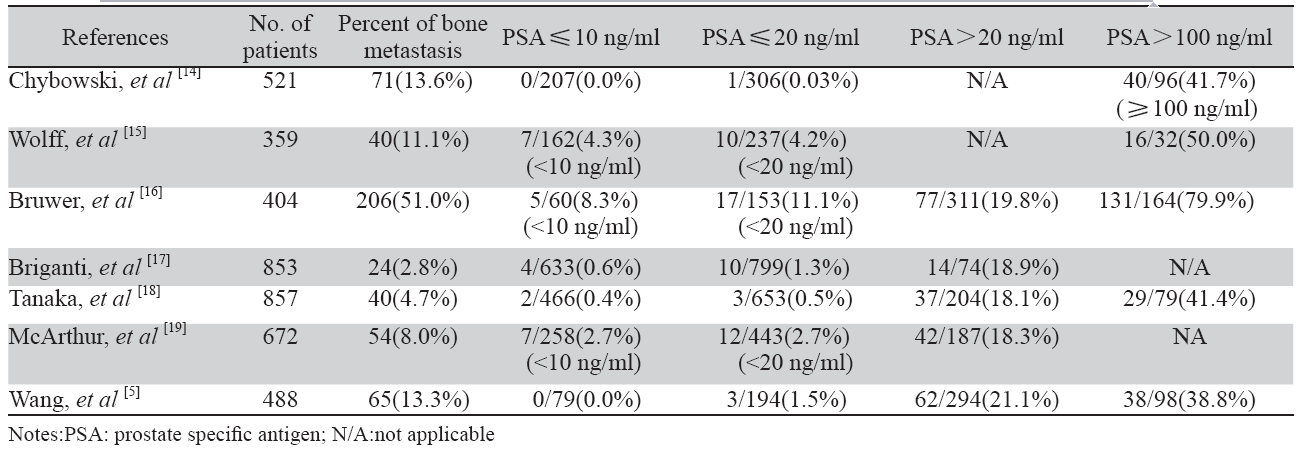
血清PSA是早期发现的前列腺癌肿瘤标志物之 一[11],它是前列腺腺泡分泌的一种糖蛋白,对前列 腺组织特异,而并非前列腺癌特异指标[12]。多年 来,人们公认应用PSA作为诊断前列腺癌骨转移的 血清标志。正常情况下有屏障将前列腺腺泡与淋巴 系统相隔,当有病变破坏屏障时,可经淋巴系统进 入血液循环,因而外周血中的PSA升高[13]。目前, PSA是判断前列腺癌患者预后和提示骨转移最重要 的血清学指标。多项研究中PSA各区段的骨扫描阳 性率不同,见表1。结果显示PSA>100 ng/ml的患 者发生骨转移的比例大于38.8%,需要高度怀疑已 经发生骨转移。虽然PSA≤20 ng/ml的患者发生骨 转移的比例较低,但是每个研究中都能观察到这 个区间段里的骨转移患者。Birtle等[20]认为原因可 能是这些患者的前列腺癌组织分化较差,丧失PSA 的产生能力,致PSA表达能力低。
|
|
表1 前列腺癌患者PSA各区段骨扫描阳性率 Table 1 The proportion of positive bone metastasis at each cut-off value of PSA in patients with prostate cancer |
另外,有研究发现fPSA/tPSA比值与前列腺癌 骨转移也有相关性。王开乐等[21]研究发现骨转移 患者的fPSA/tPSA比值的均值为0.20,相较未发生 骨转移的患者显著降低;多发骨转移患者的fPSA/ tPSA比值的均值为0.12,相较单发骨转移患者显著 降低。谭维琴等[22]也获得了类似的研究结果,他 们观察到PSA>20 ng/ml同时伴有fPSA/PSA<0.18的 前列腺癌患者骨转移的阳性率极高。
近年来许多研究发现,对前列腺癌患者进行 血清PSA、病理Gleason评分综合评估比单独依靠PSA更有优势。Brigant等[17]研究认为中危(Gleason 评分≤7,临床分期T2/T3且PSA >10)和高危 (Gleason评分≥8)的患者需要在初次诊断时进行骨 扫描。McArthur等[19]表示PSA<20并且Gleason评分 <8的初次诊断患者不做骨扫描是安全的。Tanaka 等[18] 认为Gleason评分≥4+3并且PSA >50 ng/ml的 患者要强烈怀疑有骨转移。Wang等[5]研究发现, 对于我国的T1~T3期前列腺癌患者:若Gleason评 分≤3+4,则PSA>132 ng/ml时建议骨扫描;若 Gleason评分≥4+3,则PSA>44.5 ng/ml时建议骨扫 描。对于T4期的患者则骨扫描必不可少。杨桂凤 等[23]研究表明前列腺癌患者骨转移发生率与分化 程度、血清PSA值有一定关系,低分化(Gleason评 分>7)或PSA>20 ng/ml发生骨转移可能性越大。 2 血清碱性磷酸酶
碱性磷酸酶(alkaline phosphatase,ALP)是较 早应用于临床检测前列腺癌骨转移的生化指标。 Lorente等[24]与Wymenga等[25]研究都发现,血清 ALP水平与骨显像的结果有非常好的相关性。张俊 等[26]认为ALP对于治疗前的前列腺癌在诊断骨转移 的效能高于PSA,其升高的程度与骨转移的严重程 度相关。
ALP分为六种同功酶,分别来源于肝脏、骨 骼、胎盘及小肠等,来源于骨骼的主要是ALP-3 又叫骨源性碱性磷酸酶(bone alkaline phosphatase, BALP)。在PSA、ALP、BALP诊断骨转移中, BALP敏感度最低但是特异性最高。李振雪[27]认为 BALP的这个特点正好可以与敏感度高、特异性低 的骨显像相互弥补不足,将两者联合应用是理想 的选择。张晓丽等[28]发现将BALP与fPSA/tPSA联 合应用,也可以起到互补的效果。 3 抗酒石酸酸性磷酸酶5b
骨吸收标志物抗酒石酸酸性磷酸酶5b(tartrateresistant acid phosphatase 5b,TRACP 5b)由破骨细 胞分泌,能反映破骨细胞活性,指示骨骼代谢的 变化。在病理情况下,包括骨转移时,由于破骨 细胞活性增加,血清TRACP 5b浓度显著升高。 Salminen等[29]研究发现血清TRACP 5b与PSA预测 前列腺癌骨转移的准确度相当,以4.89 u/L作为临 界值,敏感度、特异性分别达到76%和89%。楼慧 玲等[30]以4.0 u/L作为血清TRACP 5b的临界值,发 现其预测前列腺癌骨转移的敏感度、特异性分别 达到59.3%和79.7%。Ozu等[31]报告联合应用PSA、 ALP、TRACP 5b的多因素回归模型可以准确预测 前列腺癌骨转移,有70%的患者使用这个预测模型 可以代替骨扫描检查。 4 Ⅰ型胶原吡啶交联终肽
血清Ⅰ型胶原吡啶交联终肽(carboxy-terminal pyridinoline cross-linked telopeptide parts of type-Ⅰ collagen,1CTP)是另一个骨吸收标志物,是由细胞 外的金属蛋白酶介导的Ⅰ型胶原蛋白分解产物, 对病理性的骨质破坏有特异性,与TRACP 5b联 合有利于鉴别生理性骨质疏松[32]。楼慧玲等[30]以 4.3u/L作为血清1CTP的临界值,发现其预测前列 腺癌骨转移的敏感度和特异性分别达到37.0%和 80.0%。Kamiya等[33]研究认为1CTP在预测前列腺 癌骨转移的指标中是最可靠的,而且1CTP是唯一 能独立预测骨转移患者生存预后的血清标志物。 5 其他血清标志物
骨保护素(osteoprotegerin,OPG)是成骨细胞产 生的成骨性因子,可引起成骨性改变,陈海昕等[34] 发现血清OPG在前列腺癌患者体内与前列腺特异 性抗原和碱性磷酸酶浓度呈正相关(P<0.001);与 Gleason评分和病理分级呈正相关(P=0.001)。受试 者工作特征(ROC)曲线分析,OPG的曲线下面积 (AUC)较碱性磷酸酶大,对骨转移的诊断价值高。
王亚萍等[35] 用电化学发光免疫分析检测血 清Ⅰ型胶原羧基端肽β特殊序列(c-terminal crosslinking telopeptide of type Ⅰ collagen,β-CTX)和总 Ⅰ型胶原氨基端延长肽(total type Ⅰ procollagen N-terminal peptide,Total-P1NP)水平,发现前列腺癌 骨转移组的血清β-CTX明显高于无骨转移组及正常 对照组(P<0.05),而血清Total-P1NP明显低于无骨 转移组及正常对照组(P<0.05)。β-CTX在体内日间变异系数<10%,明显低于其他评价骨吸收的生化 指标,同时还可预示骨折发生的风险,具有很好 的应用前景[36]。
金玮等[37]观察到有骨转移前列腺癌患者血浆 中转化生长因子β1(transforming growth factorβ1, TGF-β1) 与无骨转移前列腺癌患者相比明显升高(P <0.05),提示血浆TGF-β1水平有助于肿瘤骨转移 的诊断。
刘洪宇等[38] 采用表面增强激光解析电离飞行 时间质谱技术筛选前列腺癌骨转移血清差异性相 关蛋白质,发现前列腺癌无骨转移组在质荷比为 2 089、4 281、3 507、4 178处的蛋白质的相对含 量明显高于前列腺癌骨转移组;前列腺癌无骨转 移组在质荷比为15 900、16 081处的蛋白质的相对 含量明显低于前列腺癌骨转移组。通过蛋白芯片 仪发现的差异性相关蛋白质,有望成为前列腺癌骨 转移诊断中有应用价值的临床检测指标。 6 总结与展望
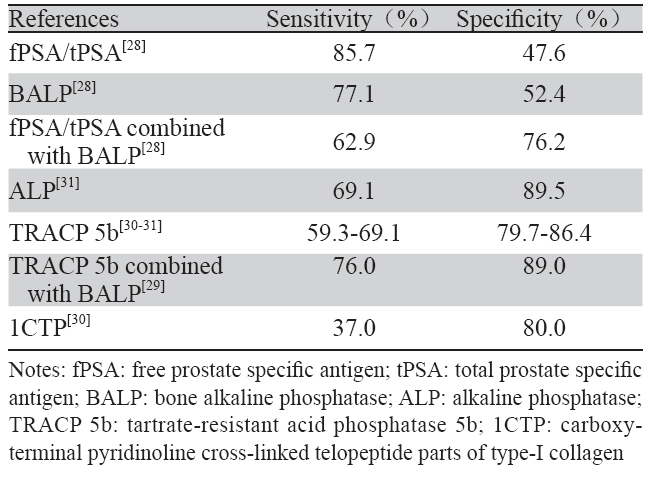
血清学指标与核素骨显像检查比较,有特异 性高、无放射性、便于随访的特点。近年来,国 内外一些研究,采用多种血清学指标联合Gleason 评分、临床T分期等临床特征,建立多因素回归 模型[5, 17, 18]预测骨转移的发生。Tanaka等[18]用上述 预测模型筛查前列腺癌患者,筛选出骨转移危险 度低的患者不进行骨扫描也是安全的,这样可以 减少患者进行骨显像的次数。血清指标如PSA、 fPSA/tPSA、ALP、BALP、TRACP 5b和1CTP都 能确切地帮助早期诊断前列腺癌的骨转移。前列 腺癌患者血清标志物的敏感度、特异性,见表2。 上述指标又各自具有不同的特点,联合应用能互相弥补不足,未来可以加入多因素回归预测模型令 预测结果更准确。其他血清指标如OPG、β-CTX 、 TGF-β1和血清差异性相关蛋白质也与前列腺癌骨 转移有很好的相关性与应用前景,但相关研究报 道不多,它们的价值有待更大样本量的研究来进 一步判断。
|
|
表2 前列腺癌患者血清标志物敏感度和特异性 Table 2 Sensitivity and specificity of serum markers in patients with prostate cancer |
| [1] | Li M, Zhang SW, Ma JH, et al. A comparative study on incidence trends of prostate cancer in part of cities and counties in China[J]. Zhonghua Mi Niao Wai Ke Za Zhi,2009,30(6):368-70. [李鸣,张 思维,马建辉,等. 中国部分市县前列腺癌发病趋势比较研究[J]. 中华泌尿外科杂志, 2009,30(6):368-70.] |
| [2] | Ye DW, Li CL.Epidemiological trends of prostate cancer: retrospect and prospect[J]. Zhongguo Ai Zheng Za Zhi,2007,17(3):177-80.[叶 定伟,李长岭.前列腺癌发病趋势的回顾和展望[J]. 中国癌症杂 志,2007,17(3):177-80.] |
| [3] | Center MM, Jemal A, Lortet-Tieulent J, et al. International variation in prostate cancer incidence and mortality rates[J]. Eur Urol,2012,61(6):1079-92. |
| [4] | Ma CG, Ye DW, Li CL, et al. Epidemiology of prostate cancer from three centers and analysis of the first-fine hormonal therapy for the advanced disease[J]. Zhonghua Wai Ke Za Zhi,2008,46(12):921-5. [马春光,叶定伟,李长岭,等. 列腺癌 的流行病学特征及晚期一线内分泌治疗分析[J]. 中华外科杂 志,2008,46(12):921-5.] |
| [5] | Wang Y, Guo J, Xu L, et al. Should bone scan be performed in Chinese prostate cancer patients at the time of diagnosis?[J]. Urol Int,2013,91(2):160-4. |
| [6] | Groot MT, Boeken Kruger CG, Pelger RC, et al. Costs of prostate cancer, metastatic to the bone, in the Netherlands[J]. Eur Urol,2003,43(3):226-32. |
| [7] | Carlin BI, Andriole GL. The natural history, skeletal complications, and management of bone metastases in patients with prostate carcinoma[J]. Cancer,2000,88(12 Suppl):2989-94. |
| [8] | Rigaud J, Tiguert R, Le Normand L, et al. Prognostic value of bone scan in patients with metastatic prostate cancer treated initially with androgen deprivation therapy[J]. J Urol,2002,168(4 Pt 1):1423-6. |
| [9] | Hsieh YY, Tsai HD, Chang FC. Routine blastocyst culture and transfer: 201 patients’ experience[J]. J Assist Reprod Genet,2000,17(8):405-8. |
| [10] | Na YQ. Guideline to diagnosis and treatment of urological diseases China[Z]. Beijing: People's Health Publishing House, 2011. [那彦 群.中国泌尿外科疾病诊断治疗指南[Z].北京:人民卫生出 版社,2011.] |
| [11] | Lamb DS, Slaney D, Smart R, et al. Prostate cancer: the new evidence base for diagnosis and treatment[J]. Pathology,2007,39( 6):537-44. |
| [12] | Wang Z,Zhou LQ,Gao JP,et al. Combination of prostate specifi c antigen and pathological stage regarding to gleason score to predict bone metastasis of newly diagnosed prostate cancer[J]. Biao Ji Mian Yi Fen Xi Yu Lin Chuang,2004,11(4):219-21.[王振, 周立权,高江平,等.血清PSA结合病理分级预测前列腺癌骨转移[J].标记免疫分析与临床,2004,11(4):219-21.] |
| [13] | Geng DZ. Chinese Geriatrics[M]. Beijing: People’s Health Publishing House, 2002:798.[耿德章. 中国老年医学[M]. 北京: 人民卫生出版社,2002:798.] |
| [14] | Chybowski FM, Keller JJ, Bergstralh EJ, et al. Predicting radionuclide bone scan fi ndings in patients with newly diagnosed, untreated prostate cancer: prostate specifi c antigen is superior to all other clinical parameters[J]. J Urol,1991,145(2):313-8. |
| [15] | Wolff JM, Zimny M, Borchers H, et al. Is prostate-specifi c antigen a reliable marker of bone metastasis in patients with newly diagnosed cancer of the prostate?[J]. Eur Urol,1998,33(4):376-81. |
| [16] | Bruwer G, Heyns CF, Allen FJ. Influence of local tumour stage and grade on reliability of serum prostate-specific antigen in predicting skeletal metastases in patients with adenocarcinoma of the prostate[J]. Eur Urol,1999,35(3):223-7. |
| [17] | Briganti A, Passoni N, Ferrari M, et al. When to perform bone scan in patients with newly diagnosed prostate cancer: external validation of the currently available guidelines and proposal of a novel risk stratifi cation tool[J]. Eur Urol,2010,57(4):551-8. |
| [18] | Tanaka N, Fujimoto K, Shinkai T, et al. Bone scan can be spared in asymptomatic prostate cancer patients with PSA of ≤20 ng/ml and Gleason score of ≤6 at the initial stage of diagnosis[J]. Jpn J Clin Oncol,2011,41(10):1209-13. |
| [19] | McArthur C, McLaughlin G, Meddings RN. Changing the referral criteria for bone scan in newly diagnosed prostate cancer patients[J]. Br J Radiol,2012,85(1012):390-4. |
| [20] | Birtle AJ, Freeman A, Masters JR, et al. Clinical features of patients who present with metastatic prostate carcinoma and serum prostate-specifi c antigen (PSA) levels < 10 ng/mL: the “PSA negative” patients[J]. Cancer,2003,98(11):2362-7. |
| [21] | Wang KL, Song LP. The diagnostic value of combining whole body bone images with serum PSA, fPSA and fPSA/PSA ratio in the diagnosis of bone metastasis in patients with prostate cancer[J]. Zhongguo Lin Chuang Yi Xue Ying Xiang Za Zhi,2012,23(9):672-4. [王开乐,宋丽萍. 全身骨显像联合血清 PSA、fPSA及fPSA/PSA比值对前列腺癌骨转移的诊断价值[J]. 中国临床医学影像杂志,2012,23(9):672-4.] |
| [22] | Tan WQ, Yang SJ. Analysis of relationship between serum PSA, fPSA levels and bone metastasis in prostatic cancer[J]. Fang She Mian Yi Xue Za Zhi,2007,20(2):160-2. [谭维琴,杨士军. 血清 PSA、fPSA浓度与前列腺癌骨转移的关系分析[J]. 放射免疫学 杂志,2007,20(2):160-2.] |
| [23] | Yang GF, Zuo SY, Wang GM, et al. Research of whole bone scanning in the diagnosis of metastatic diseases in prostate cancer, and its correlation with pathological grade and PSA[J]. Zhongguo Lin Chuang Yi Xue Ying Xiang Za Zhi, 2010,21(1):72-3. [杨 桂凤,左书耀,王国明,等. 骨显像诊断前列腺癌骨转 移与病理分级及PSA的关系探讨[J]. 中国临床医学影像杂 志,2010,21(1):72-3. |
| [24] | Lorente JA, Valenzuela H, Morote J, et al. Serum bone alkaline phosphatase levels enhance the clinical utility of prostate specifi c antigen in the staging of newly diagnosed prostate cancer patients[J]. Eur J Nucl Med,1999,26(6):625-32. |
| [25] | Wymenga LF, Boomsma JH, Groenier K, et al. Routine bone scans in patients with prostate cancer related to serum prostate-specifi c antigen and alkaline phosphatase[J]. BJU Int,2001,88(3):226-30. |
| [26] | Zhang J, Liu ZL, Cui XJ, et al. The application of radionuclide bone scintigraphy,serum PSA and ALP measurement in diagnosis of bone metastasis in prostate cancer patients[J]. Suzhou Da Xue Xue Bao(Yi Xue Ban),2007,27(3):407-10. [张俊,刘 增礼,崔学军,等. 核素骨显像和血清PSA、ALP检测在 前列腺癌骨转移诊断中的价值[J]. 苏州大学学报(医学 版),2007,27(3):407-10.] |
| [27] | Li ZX. The clinical importance on detecting the BALP in prostatic carcinoma complicating osseous metastasis patients[J]. Zhongguo Shi Yan Zhen Duan Xue,2006,10(9):1074-6.[ 李振 雪. BALP在前列腺癌骨转移中的检测意义[J]. 中国实验诊断 学,2006,10(9):1074-6.] |
| [28] | Zhang XL,Zhang JS,Zhang JK, et al. The diagnostic value on detecting the BALP and f-PSA/t-PSA in patients with bone metastasis of prostatic cancer[J]. Zhongguo Shi Yan Zhen Duan Xue,2009,13(10):1381-3.[ 张晓丽,张吉生,张敬凯,等. BALP与f-PSA/t-PSA联合检测对前列腺癌骨转移诊断价值的 研究[J]. 中国实验诊断学,2009,13(10):1381-3.] |
| [29] | Salminen E, Ala-Houhala M, Korpela J, et al. Serum tartrateresistant acid phosphatase 5b (TRACP 5b) as a marker of skeletal changes in prostate cancer[J]. Acta Oncol,2005,44(7):742-7. |
| [30] | Luo HL, Chen QC. Signifi cance of prostate specifi c antigen and markers of bone formation or resorption in diagnosis of bone metastasis of prostate cancer[J]. Zhonghua Lao Nian Yi Xue Za Zhi,2012,31(5):421-4.[ 楼慧玲,陈巧聪. 前列腺特异性抗原及 骨标志物检测对前列腺癌骨转移患者诊断的意义[J]. 中华老年 医学杂志,2012,31(5):421-4.] |
| [31] | Ozu C, Nakashima J, Horiguchi Y, et al. Prediction of bone metastases by combination of tartrate-resistant acid phosphatase, alkaline phosphatase and prostate specifi c antigen in patients with prostate cancer[J]. Int J Urol,2008,15(5):419-22. |
| [32] | Korpela J, Tiitinen SL, Hiekkanen H, et al. Serum TRACP 5b and ICTP as markers of bone metastases in breast cancer[J]. Anticancer Res,2006,26(4B):3127-32. |
| [33] | Kamiya N, Suzuki H, Yano M, et al. Implications of serum bone turnover markers in prostate cancer patients with bone metastasis[J]. Urology,2010,75(6):1446-51. |
| [34] | Chen HX, Li HZ, Li HJ, et al. Serum osteoprotegerin as a novel marker of bone metastasis in prostate cancer[J]. Zhonghua Wai Ke Za Zhi,2007,45(6):412-4.[ 陈海昕,李汉忠,李宏军,等. 血清骨保护素诊断前列腺癌骨转移的初步研究[J]. 中华外科杂 志,2007,45(6):412-4.] |
| [35] | Wang YP,Huang X, Lu ZX. Significance of the β-CTX and P1NP combined detection in the diagnose of osseous metastasis of prostatic carcinoma[J]. Fang She Mian Yi Xue Za Zhi,2011,24(4):435-7.[ 王亚萍,黄璇,卢志贤. 血清β-CTX和 Total-P1NP联检在前列腺癌骨转移监测中的价值[J]. 放射免疫 学杂志,2011,24(4):435-7.] |
| [36] | Wang LJ, Fu HP. The clinical application of serum β-Crosslaps determination[J]. Jian Yan Yi Xue,2007,22(6):633-5.[ 王立军, 傅海平. 血清β-胶原特殊序列的测定及初步临床应用[J]. 检验 医学,2007,22(6):633-5]. |
| [37] | Jin W, Wu B, Zhang H. Clinical significance of TGF-β1 levels change in prostate cancer patients[J]. Shandong Yi Yao,2011,51(42):63-4.[ 金玮,吴斌,张辉. 前列腺癌患者血浆 TGF-β1水平变化及临床意义[J]. 山东医药,2011,51(42):63-4.] |
| [38] | Liu HY,Mi ZG, Han XB, et al. Identifi cation of serum protein of prostate cancer with osseous metastasis[J]. Zhong Liu Yan Jiu Yu Lin Chuang,2011,23(3):197-200. [ 刘洪宇,米振国,韩雪冰, 等. 前列腺癌骨转移患者血清差异性相关蛋白质的筛选[J]. 肿 瘤研究与临床,2011,23(3):197-200.] |